 Owner income$130k-$1.41M
Owner income$130k-$1.41MHow Much Does a Physiotherapy Clinic Owner Make? $130k–$141M

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$130k-$1.41M  Net margin-94% to 479%
Net margin-94% to 479% Revenue for target pay$38.2k-$222.7k
Revenue for target pay$38.2k-$222.7k Business difficultyHard
Business difficultyHard


A physiotherapy clinic owner can earn a $130,000 clinic director salary in the first year in this model, but the clinic itself shows a -$43,074 operating loss before reserves, debt service, and personal taxes By Year 2, revenue reaches about $840,696 with $125,767 in operating profit, creating potential owner income of about $255,767 before reserves if the owner also takes distributions By Year 5, the model reaches $2,672,760 in revenue and $1,280,577 in operating profit, but that is not guaranteed cash take-home
Owner income$130k-$1.41MNet margin-94% to 479%Revenue for target pay$38.2k-$222.7kBusiness difficultyHardWant to test your own clinic income?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner income is not guaranteed and this is not tax advice or owner distribution advice.
Want the full Physiotherapy Clinic forecast?
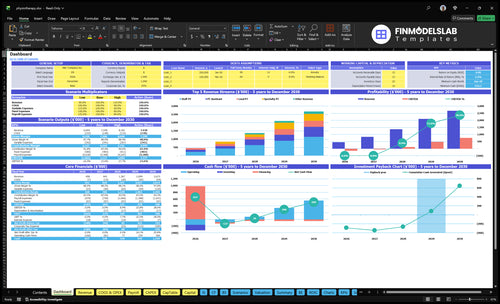
The Physiotherapy Clinic Financial Model Template maps revenue, costs, cash flow, and owner take-home; it also shows visit volume, provider count, capacity ramp, and scenario testing. It’s a planning aid, not a promise of earnings or payer reimbursement.
Model highlights
- Owner income outputs
- Revenue and margin charts
- Scenarios and assumptions
What affects physical therapy clinic profit margin?
For a Physiotherapy Clinic, payroll and utilization move profit margin first; for setup cost context, see How Much Does It Cost To Open A Physiotherapy Clinic?. Year 1 payroll is $375,000 against $458,280 revenue, so margin is -94%, while Year 5 payroll is $1,125,000 against $2,672,760 revenue, so margin rises to 479% before reserves and taxes. Fixed overhead is $8,050/month, so small shifts in reimbursement, billing fees, or empty schedules can change owner take-home fast.
Margin drivers
- Payroll hits margin first
- Utilization sets revenue capacity
- Reimbursement changes take-home
- Empty schedules cut profit fast
Fixed overhead
- $5,000 rent each month
- $800 utilities each month
- $500 electronic health record software
- $300 liability insurance
How much revenue does a physical therapy clinic need to pay the owner?
A Physiotherapy Clinic needs about $840,696 in Year 2 annual revenue to support a $125,767 operating profit before reserves, while Year 1 revenue of $458,280 is not enough to cover all listed costs. It can pay a $130,000 clinic director salary from launch, but owner target pay is not the same as cash available because reserves, debt service, equipment, and reinvestment come before distributions.
Revenue target
- $840,696 Year 2 revenue target
- $125,767 profit before reserves
- $458,280 Year 1 revenue
- Year 1 does not cover all costs
Owner pay logic
- $130,000 clinic director salary from launch
- Work backward from owner target pay
- Include payroll, billing, consumables
- Reserves come before distributions
How many patients does a physiotherapy clinic need to make money?
A Physiotherapy Clinic starts making money at about 147 completed visits per week in this model; 88 completed visits per week still loses $43,074 in Year 1. Read What Is The Primary Goal Of The Physiotherapy Clinic? to keep the target tied to completed treatments, not booked appointments. Here’s the quick math: Year 2 earns $125,767 on about 7,644 annual visits, or roughly $16 per completed visit after listed expenses.
Profit target
- Year 1: 88 visits/week
- Year 1 loss: $43,074
- Year 2: 147 visits/week
- Year 2 profit: $125,767
Watch risks
- Track completed visits first
- Control cancellations and no-shows
- Match therapists to room capacity
- Referrals lag; payroll still repeats
Want the six income drivers that matter most?
1
440-800/moVisit Volume
More completed visits lift revenue fast; the model grows from 440 treatments a month in Year 1 to 800 in Year 5.
2
$80-$150Collections Mix
Mixing Lead PT, Staff PT, Specialty PT, Wellness Coach, and Assistant visits changes what the clinic collects per treatment.
3
60%-88%Provider Utilization
Fuller schedules raise revenue from the same team, with utilization moving from 60% to 88% by role.
4
$415K-$1.26MCost Control
Payroll is the biggest cost block, and fixed overhead plus fees still matter, so headcount discipline protects take-home pay.
5
26 moReferral Retention
Stronger referrals and repeat visits shorten the path to breakeven, which the model reaches in Month 26.
6
1-2 PTsOwner Scaling
The owner's clinical role sets how fast the clinic can grow without capping volume or quality.
Physiotherapy Clinic Core Six Income Drivers
Completed Visit Volume
Completed Visit Volume
Completed visits drive cash because the clinic only gets paid when care is delivered, not when a patient calls or books. The model rises from 380 completed visits per month in Year 1 to 1,906 in Year 5, or from 88 weekly visits to 440. That is about 5x growth, so every filled slot matters for revenue and owner pay.
Here’s the catch: cancellations, no-shows, therapist availability, room capacity, and schedule discipline decide whether paid capacity turns into collections. Empty slots hurt twice because payroll and rent still run. If visits do not convert, gross profit falls fast and the owner has less cash left for draws, taxes, and reserves.
Track and fill the schedule
Measure scheduled visits, completed visits, cancellation rate, no-show rate, and hours booked per provider. The key formula is simple: completed visits = scheduled visits minus cancels minus no-shows. If the schedule is weak, the clinic can look busy on paper but still miss cash.
Set daily fill targets by therapist and room, then review gaps every week. Track which referral sources produce kept visits, not just booked visits. If completion drops, tighten reminders, confirm insurance, and cut open slots before fixed costs like $8,050 per month keep draining profit.
- Count kept visits, not bookings.
- Watch no-shows by provider.
- Fill gaps within 24 hours.
- Compare room time to paid time.
1
Average Collections And Payer Mix
Average Collections And Payer Mix
Average collected revenue per visit is the driver here, not billed charges. In Year 1, modeled prices are $125 for Lead PT, $105 for Staff PT, and $80 for PT Assistant. In Year 5, the mix rises to $140, $120, $150 for Specialty PT, $90 for Wellness Coach, and $95 for PT Assistant, so the same visit count can produce more cash and a bigger owner draw.
Here’s the quick math: moving one visit from PT Assistant at $80 to Lead PT at $125 adds $45 collected revenue. If payer mix slips, cash falls even when schedules stay full. Model collections from contracts, documentation, denied claims, and cash-pay visits, because unpaid charges do not help profit or payroll.
Measure Net Collections Per Visit
Track collections by provider type, payer, and visit type. Watch net collected per completed visit, not charges, and compare it to schedule templates each month. If a service line pays more but collects slower, cash flow can still tighten. One clean rule: better mix beats higher volume when overhead is fixed.
- Net collections per visit
- Payer denial rate
- Cash-pay share
- Collected dollars by provider
2
Provider Utilization And Staffing
Provider Utilization
Owner income rises when paid provider hours turn into completed reimbursable visits. Here, Lead PT utilization moves from 60% to 85%, Staff PT from 65% to 88%, and PT Assistant from 70% to 88%. That lifts collections because the clinic earns from billed care, not idle schedule time.
The staffing mix also changes, from 1 clinic director, 2 Staff Physical Therapists, and 1 Physical Therapy Assistant to a larger multi-provider team. Higher utilization can raise gross profit, but the safe limit is set by supervision, care quality, and documentation. If those slip, more booked hours do not become paid visits.
Track Billable Hours
Measure utilization by provider each week: completed visits ÷ paid clinical hours. Watch the gap between scheduled time and billed time, plus cancellations, no-shows, and documentation lag. A clinic can look busy and still miss cash if those hours do not close into reimbursable visits.
Build staffing to protect quality, not just volume. The useful test is simple: if utilization rises but patient outcomes, supervision, or charting quality falls, stop there. For planning, use the target steps of 60% to 85%, 65% to 88%, and 70% to 88% as the operating benchmark, then forecast owner pay from the visits those hours can realistically support.
- Track utilization by clinician weekly.
- Count completed reimbursable visits only.
- Monitor no-shows and cancellations.
- Check supervision and chart quality.
- Test staffing before adding more hours.
3
Operating Costs And Overhead
Overhead and Take-Home Pay
If overhead stays high, the clinic can be busy and still leave little for the owner. Fixed costs are $8,050/month before variable fees or treatment supplies. That includes rent, utilities, electronic health record software, liability insurance, office supplies, website and digital tools, cleaning, and accounting and legal. Those bills hit every month, so they set the floor for break-even cash.
Then come the variable costs: 50% of revenue in Year 1 and 45% by Year 5, plus consumables from $150 to $220 per completed treatment. That means higher visit volume helps, but only if collections rise faster than cost per visit. If cancellations or low reimbursement cut revenue, owner pay shrinks fast because overhead still runs.
Track Cost per Visit
Measure overhead as fixed cost per completed visit and as a share of collections. The key inputs are monthly revenue, completed visits, payer mix, and treatment supply use. Here’s the quick math: more visits spread the $8,050 fixed base wider, but each visit still carries variable fees and consumables, so margin only improves when collections outpace those costs.
- Fixed overhead: rent, utilities, software
- Variable fees: 50% then 45%
- Consumables per visit: $150 to $220
- Net cash after overhead: owner draw and reserves
If consumables drift toward $220 per treatment or a service mix uses more supplies, margin drops even when revenue holds steady. Set monthly limits, review vendor spend, and price to protect contribution. The rule is simple: control cost per visit first, then decide what remains for reserves and owner income.
4
Referral Pipeline And Patient Retention
Referral Pipeline And Retention
A steady referral and retention system keeps the schedule full enough to pay the owner. The model needs about 88 weekly visits in Year 1, 147 in Year 2, and 440 in Year 5, so weak flow shows up fast in cash. If visits fall short, salari es, rent, software, and insurance still keep running.
This driver includes physician referrals, direct access awareness, reviews, local search, patient experience, and completed plans of care. More completed visits means more collections, better margin coverage, and less empty time. One clean rule: empty slots hurt twice because revenue drops and fixed overhead stays put.
Track Weekly Fill And Rebooking
Track weekly completed visits against the path, plus referral source, no-show rate, and plan completion rate. Here’s the quick math: if the clinic misses the 88 to 147 weekly ramp, the owner’s income base shrinks before costs move. Watch physician relationships, direct access awareness, reviews, and local search together.
- Weekly visits vs target
- New referrals by source
- Plan completion rate
- Cancel and no-show rate
Use reminders, fast rebooking, and clear home plans so patients finish care. If retention slips, the clinic loses margin now and leaves fewer visits to absorb fixed overhead. The goal is simple: keep the calendar full enough that owner pay comes from real collected visits, not from hoped-for demand.
5
Owner Role And Scaling Strategy
Owner Role Sets the Pay Curve
A treating owner can support early revenue because their own visits create collections. Once the owner becomes a managing owner, income depends on hired therapists, utilization, supervision, and schedule fill. In Year 1, the model includes a $130,000 clinic director salary but still shows negative operating profit, so owner pay can outrun cash flow before the clinic is scaled.
By Year 5, operating profit reaches $1,280,577 before reserves and taxes, but that requires a much larger team. The hidden risk is simple: if therapist hours, room time, and completed visits do not rise together, added management costs and hiring gaps can cut the owner’s take-home income fast.
Track Utilization Before You Add Headcount
Measure completed visits per provider, visit fill rate, cancellations, no-shows, and supervision time. Those inputs decide whether a new hire adds profit or just adds payroll. A treating owner can keep cash coming in; a managing owner needs a repeatable system that keeps each clinician busy enough to cover salary, rent, and admin overhead.
Before opening a second location or adding more providers, test the math on staffing cost, manager cost, and reinvestment needs. If one clinician can’t hold target utilization, scaling usually widens losses first. The safe move is to hire against booked demand, not hope, and keep the owner’s role clear: treat, manage, or both.
6
Scenario objective: compare lean, base, and high physiotherapy clinic owner-income outcomes
Owner income scenarios
Owner income changes fast as visit volume, staffing, and service mix scale. Early months look salary-led, while later years can add profit draws if the clinic hits modeled capacity.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | This is the lean income case with early-stage volume and no supported profit distribution. | This is the modeled middle case with salary plus a profit draw as volume improves. | This is the stronger earnings path if the clinic reaches high volume and a broader service mix. |
| Typical setup | At 88 weekly visits and $458,280 in annual revenue, the clinic is still in a loss phase, so owner income is limited to the $130,000 salary. | At 147 weekly visits and $840,696 in annual revenue, the clinic supports $125,767 of operating profit and about $255,767 of owner income before reserves. | At 440 weekly visits and $2,672,760 in annual revenue, the clinic reaches $1,280,577 of operating profit and about $1,410,577 of owner income before reserves. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $130,000Salary only | $255,767Salary plus profit | $1,410,577High upside |
| Best fit | Use this to stress-test the first operating year and cash needs. | Use this for main planning and lender conversations. | Use this to test upside and hiring pressure at scale. |
Planning note: These scenario figures are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Physiotherapy Clinic Porter's Five Forces Analysis
- Physiotherapy Clinic BCG Matrix
- Physiotherapy Clinic Business Model Canvas
- 7 Critical KPIs to Measure for a Physiotherapy Clinic
- Physiotherapy Clinic Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Physiotherapy Clinic Profitability
- How Much Does It Cost To Run A Physiotherapy Clinic Monthly?
- Physiotherapy Clinic Startup Costs: $75k Build-Out, $50k Equipment
- Physiotherapy Clinic Financial Model Template in Excel
- How To Open A Physiotherapy Clinic In 4 To 9 Months
- How to Write a Physiotherapy Clinic Business Plan in 7 Steps
- Physiotherapy Clinic Marketing Mix
- Physiotherapy Clinic Marketing Plan
- Physiotherapy Clinic Business Proposal
- Physiotherapy Clinic PESTEL Analysis
- Physiotherapy Clinic Pitch Deck Example Editable PPTX
- Physiotherapy Clinic Business SWOT Analysis
- Physiotherapy Clinic Value Proposition Canvas
Frequently Asked Questions
In this model, the owner earns a $130,000 clinic director salary in Year 1, but the clinic loses $43,074 before reserves and taxes By Year 2, operating profit reaches $125,767 on $840,696 revenue If the owner takes salary plus available profit, potential income is $255,767 before reserves