 Owner income$227,346
Owner income$227,346How Much Radiology Center Owners Make: $227K Year 1 EBITDA View

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$227,346  Net margin118%–480%
Net margin118%–480% Revenue for target pay$160,925–$563,793
Revenue for target pay$160,925–$563,793 Business difficultyHard
Business difficultyHard



Key Takeaways
- Revenue comes from completed studies, not bookings.
- MRI and CT lift revenue, but raise costs.
- A 5% collection swing shifts about $96,555 yearly.
- Payroll starts at $1,020,000 and sets break-even.
Owner income$227,346Net margin118%–480%Revenue for target pay$160,925–$563,793Business difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Not guaranteed salary, tax advice, or owner distribution advice.
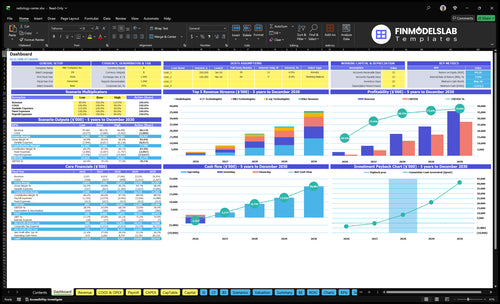
Want to see the forecast in the Radiology Center Radiology Center Financial Model Template?
See the Radiology Center dashboard for revenue, EBITDA, margin, and owner cash; open the model.
Owner-income model highlights
- Owner cash after reserves
- Revenue, EBITDA, margin
- Year 1 to Year 4
How much revenue does a radiology center need for owner pay?
A Radiology Center needs about $138,895 a month in revenue to cover the $119,450 fixed overhead and payroll base before debt service, reserves, and owner pay. Year 1 revenue is $160,925 a month, so the cushion is only about $22,030. At the same margin, each extra $10,000 of owner draw, debt service, or reserves needs about $11,628 more monthly revenue.
Core math
- $119,450 monthly fixed base
- $138,895 break-even revenue
- $160,925 Year 1 revenue
- $22,030 revenue cushion
Owner pay impact
- $10,000 extra draw needs more revenue
- Revenue lift needed: $11,628
- Debt service uses the same math
- Reserves also use the same math
What affects radiology center profit margins the most?
For a Radiology Center, profit margin pressure starts with payroll: $1,020,000 in Year 1 staffing cost, plus $413,400 a year in fixed overhead led by $20,000 monthly rent. Variable costs also bite hard, with supplies and consumables at 55% of revenue, billing and collections at 50%, and service contracts at 35%; if you want the launch-budget context, see What Is The Estimated Cost To Open And Launch Your Radiology Center?.
Main margin drivers
- Payroll: $1,020,000 in Year 1
- Fixed overhead: $413,400 yearly
- Rent: $20,000 monthly
- 1% revenue swing: about $19,311 yearly
Cost lines to watch
- Supplies and consumables: 55% of revenue
- Billing and collections: 50% of revenue
- Service contracts: 35% of revenue
- Model equipment financing separately
How much can a radiology center owner take home?
A Radiology Center owner can’t take home gross collections; take-home starts with cash flow, and Year 1 modeled EBITDA is $227,346, or about $18,946/month, before debt service, taxes, reserves, and distributions; for context, track What Is The Most Critical Metric To Measure The Success Of Radiology Center? alongside owner pay. If equipment payments and reserves exceed EBITDA, owner distributions may be low or zero; by Year 4, EBITDA reaches $3,250,254 before financing and reserves.
Year 1 Cash
- Revenue: $1,931,100
- EBITDA: $227,346
- Monthly EBITDA: $18,946
- Payroll: $1,020,000
Distribution Limits
- Fixed overhead: $34,450/month
- Debt service comes after EBITDA
- Reserves reduce owner draws
- Year 4 EBITDA: $3,250,254
Want the six owner income drivers?
1
$161K/moScan Volume
More monthly scans lift revenue fast because fixed costs are already in place.
2
$75-$650Reimbursement Mix
MRI and CT pay far more than X-ray, so mix changes revenue per study.
3
25%-90%Uptime
If equipment or staff sit idle, those high-ticket slots never hit the schedule.
4
$1.02MPayroll
Payroll is the biggest cost block, so FTE count has a direct pull on take-home.
5
1,500/moReferral Flow
Referrals, authorizations, and no-shows decide how many booked studies actually show.
6
$34.45K/moFixed Overhead
Lease, utilities, software, and admin costs hit cash every month no matter what.
Radiology Center Core Six Income Drivers
Scan Volume And Utilization
Scan Volume And Utilization
The money comes from completed reimbursable studies, not booked appointments. In Year 1, modeled capacity of 250% to 400% supports about $160,925 in monthly revenue; by Year 4, 700% to 800% supports about $563,793 monthly. When scan volume rises faster than fixed costs, the owner’s take-home income improves because payroll, rent, and equipment overhead get spread over more billable studies.
Here’s the quick math: more completed scans lift revenue, but only if the center keeps no-shows low, scanner hours full, and turnaround fast. If booked demand does not convert to completed, authorized studies, cash does not follow. Overbooking without authorization or staffing control can backfire through denials, overtime, and delayed reports, which cuts margin and slows the point where the business can pay the owner.
Improve Completed Study Yield
Track the full funnel: referrals received, authorized, scheduled, completed, and billed. The best operating lever is conversion, not just booking count. Faster scheduling, fewer no-shows, longer scanner hours, and quicker report turnaround all raise completed volume and help fixed costs get covered sooner.
- Measure no-show rate by modality.
- Track completed studies per scanner hour.
- Watch denial and overtime costs weekly.
Use staffing and scanner slots to match actual demand, not forecasted bookings. If a modality is pushed above its staffed capacity, the hidden cost shows up fast in reschedules, slower reporting, and overtime. Keep authorization, scheduling, and staffing aligned so higher utilization turns into collected revenue and owner profit, not just busier calendars.
1
Modality Mix
Modality Mix
Modality mix changes revenue per completed study and the cost to deliver it. In Year 1, modeled prices are $580 MRI, $340 CT, and $75 X-ray, plus $140 radiologist units and $95 nurse units. MRI and CT lift revenue, but they also need trained staff, uptime, service support, and tighter cash control.
Here’s the quick math: shifting 10 studies from X-ray to MRI adds about $5,050 in billed revenue before the higher labor and equipment load. Owner income improves only when the added volume covers payroll, billing, service contracts, equipment payments, and reserves. If utilization is thin, the mix looks better on paper than in cash.
Measure Margin by Scan Type
Track gross margin per modality, not just volume. Build a monthly view of completed MRI, CT, and X-ray studies, then subtract radiologist and nurse units, billing cost, service contracts, and downtime. That tells you which scan type actually funds owner draw after fixed costs, not just which one has the highest sticker price.
Test mix changes against capacity. If MRI slots are full enough, more MRI can improve income; if uptime, staffing, or authorization slips, the margin gets eaten fast. Keep a floor on X-ray for quick throughput, and only push CT and MRI when the schedule, tech coverage, and machine support are already locked in.
2
Payer Mix And Collections
Payer Mix And Collections
Payer mix is what decides how much billed imaging revenue actually turns into cash. With service-line prices from $75 to $580 and Year 1 revenue of $1,931,100, a 5% collection swing changes annual revenue by about $96,555 and contribution by about $83,037 before staffing changes. That gap can move owner pay fast.
Model collections by payer, not one blended average. Use allowed amount, denial rate, prior authorization delays, patient balances, and days in accounts receivable for each payer type. The same scan volume can look healthy on paper and still leave the owner short on cash if commercial, Medicare, or self-pay collections land at different speeds.
Track Collections By Payer
Build a monthly report that shows billed amount, collected amount, denial rate, and days in AR by payer. Reconcile it to completed studies, not scheduled scans. A 5% miss is about $96,555 a year, so small swings in payment quality can change the owner’s draw more than a small change in volume.
Stress-test each contract against the service mix, especially the higher-priced $580 MRI and $340 CT cases. If prior auth slows, denials rise, or patient balances are harder to collect, cash comes in later even when revenue looks fine. Keep enough working cash to cover payroll, equipment, and rent before collections clear.
3
Equipment Cost And Uptime
Scanner Uptime and Debt Service
Equipment cost is a cash-flow issue, not just an accounting line. In this model, service contracts are 35% of Year 1 revenue, or about $67,589, and 32% of Year 4 revenue, or about $216,497. Any lease or loan payment sits below EBITDA, so every $1 of scanner debt service cuts owner cash by $1.
Uptime matters because downtime cuts scans while rent, payroll, insurance, and debt keep running. The key inputs are scanner hours, downtime hours, service contract cost, debt payment, and completed studies. If uptime slips, revenue falls first, then owner draw gets squeezed even when the income statement still looks fine.
Measure Downtime Before It Hits Cash
Track uptime percent, lost scan hours, and completed studies by modality. Put service contract cost, scheduled maintenance, and repair downtime into the forecast, then test the effect of a one-day outage on monthly revenue and cash. That shows how fast fixed costs eat margin when volume drops.
- Track uptime by machine.
- Log every downtime hour.
- Price debt below EBITDA.
- Reserve cash for repairs.
- Review contract terms yearly.
Use the model to see whether extra volume actually covers the added fixed load. If MRI or CT downtime rises, the owner loses revenue twice: fewer billable scans and no relief from payroll or rent. Keep spare capacity, fast service response, and a cash reserve so owner pay does not depend on perfect uptime.
4
Staffing And Read-Cost Structure
Payroll Floor
Staffing sets the break-even floor because it is a fixed cost that must be covered before owner pay starts. Year 1 payroll is $1,020,000, or about $85,000 per month, built from one radiologist at $350,000, two MRI technologists at $90,000 each, two CT technologists at $85,000 each, two X-ray technologists at $70,000 each, one radiology nurse at $80,000, and one practice manager at $100,000.
By Year 4, payroll rises to $2,290,000, or about $190,833 per month. That step-up only works if scan volume, payer collections, and scanner uptime scale faster than payroll. Owner profit is not the same as owner labor; if you work unpaid in the business, add a replacement manager cost before calling the rest profit.
Track the Labor Load
Measure payroll against collected revenue, not scheduled studies. Watch labor by modality, overtime, vacancy days, and temp coverage, becau se each empty shift or bad schedule can push fixed labor into margin loss. Keep a simple monthly view of payroll dollars per completed study and compare it with realized reimbursement by MRI, CT, and X-ray.
- Count paid clinical hours by modality.
- Separate owner labor from profit.
- Price in management replacement cost.
- Track overtime and temp staffing.
- Review payroll monthly, not quarterly.
What this model hides: if staffing runs ahead of completed scans, cash gets tight fast even when bookings look strong. The best control is matching staffing to confirmed, authorized volume and holding a margin buffer for denials, downtime, and slower collections.
5
Referral Flow And Operational Conversion
Referral-to-Billable Study Conversion
Referral flow only pays when the order becomes an authorized, completed, billable study. On a Year 1 base of $160,925 per month, every 1% of conversion lost is about $1,609 in monthly revenue, so missed scheduling, prior authorization failures, and no-shows cut owner cash fast while fixed costs keep running.
The key inputs are referral volume, authorization rate, scheduled-to-show rate, clean-order rate, report turnaround, and collection likelihood. Booked demand is not revenue until claims are likely to collect, so a full calendar can still underperform if patients never arrive or payer approval stalls.
Track the Conversion Funnel
Measure each step from referral to payment, not just booked slots. Fast scheduling, clean orders, strong report turnaround, and clear patient communication raise completed volume and protect the owner's draw.
- Referrals received vs. scheduled
- Authorization approval rate
- No-show rate by modality
- Days from scan to report
- Claims likely to collect
Use the weakest step to set staffing and slot rules. If prior auth slows or no-shows rise, add follow-up, tighten order checks, and stop counting booked demand as income until conversion is real.
6
Compare low, base, and high owner income scenarios
Owner income scenarios
Owner income changes fast as staffing, utilization, and overhead scale. These three cases show how the same center can move from a thin ramp to strong cash generation.
| Scenario | Low CaseLow Case | Base CaseBase Case | High CaseHigh Case |
|---|---|---|---|
| Launch model | This is the lower owner-income path built on Year 1 ramp assumptions. | This is the modeled middle path using Year 2 assumptions. | This is the stronger owner-income path using Year 4 assumptions. |
| Typical setup | Year 1 assumes $160,925 monthly revenue, $1,931,100 annual revenue, $1,020,000 payroll, $413,400 fixed overhead, and 140% direct plus variable costs. | Year 2 assumes $265,669 monthly revenue, $3,188,028 annual revenue, $1,615,000 payroll, and 134% direct plus variable costs. | Year 4 assumes $563,793 monthly revenue, $6,765,516 annual revenue, $2,290,000 payroll, and 120% direct plus variable costs. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $227,346Low case | $732,433Base case | $3,250,254High case |
| Best fit | Use this to stress-test a slow ramp, tighter utilization, and early cash pressure. | Use this as the core planning case for Year 2 operations and staffing. | Use this to test upside if Year 4 volume and capacity hold. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distribution forecasts.
Related Products
- Radiology Center Porter's Five Forces Analysis
- Radiology Center BCG Matrix
- Radiology Center Business Model Canvas
- 7 Critical KPIs to Track for a Radiology Center
- Radiology Center Business Plan Template in Pre-Written Word
- Increase Radiology Center Profitability: 7 Actionable Strategies
- Calculating the Monthly Running Costs for a Radiology Center
- Radiology Center Startup Costs: $385M CAPEX Planning Guide
- Radiology Center Financial Model Template in Excel
- How to Open a Radiology Center: 9–18 Month Launch Plan
- How to Write a Radiology Center Business Plan (7 Steps)
- Radiology Center Marketing Mix
- Radiology Center Marketing Plan
- Radiology Center Business Proposal
- Radiology Center PESTEL Analysis
- Radiology Center Pitch Deck Example Editable PPTX
- Radiology Center Business SWOT Analysis
- Radiology Center Value Proposition Canvas
Frequently Asked Questions
Under the modeled assumptions, Year 1 EBITDA is $227,346 on $1,931,100 of revenue, before equipment debt, taxes, reserves, and distributions That is not the same as owner salary By Year 4, EBITDA reaches $3,250,254 on $6,765,516 of revenue, assuming higher utilization and staffing are achieved