Open a Mobile Hangover IV Treatment Service in 8–16 Weeks
To open a mobile hangover IV service, line up medical governance, licensed clinical staffing, protocols, insurance, supply vendors, documentation, booking, and local demand channels before accepting appointments A practical launch path is usually 8–16 weeks, but state rules, medical director availability, insurance approval, and vendor onboarding can move that timing The researched Year 1 model assumes 28 clinicians, about 1,015 treatments per month at modeled capacity, and roughly $213,400 in monthly revenue The main bottleneck is licensed medical oversight and insurance readiness, so first revenue should come from prebooked weekend appointments, hotels, events, and local search only after capacity is ready
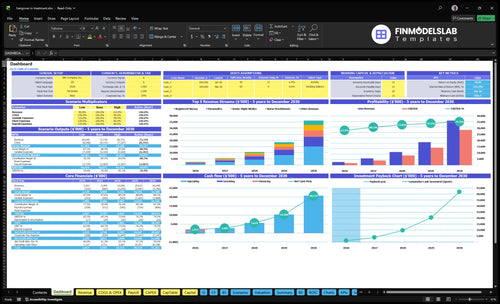
Time to Open8-16 weeksSetup windowLaunch Sequence7 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepPrebooked visitsWeekend booking
Launch timeline
This is a short web summary of the launch plan, and the XLSX export holds the detailed Gantt Chart.
What mobile IV launch mistakes create the biggest readiness risks?
The biggest readiness risk for a Hangover IV Treatment Service is launching before the safety gates are closed. If compliance, insurance, emergency protocols, documentation, and supply checks are not verified, delay launch until they are. Cost signals also matter: 105% for medical infusion supplies and IV kits, 25% for biohazard waste and sterile logistics, and 60% for practitioner travel stipends in Year 1 can squeeze cash fast.
Day-one safety gates
Verify provider oversight first
Confirm insurance and consent
Set screening and escalation rules
Use sharps disposal on day one
Operational launch risks
Do not overbook nurses
Set supply reorder points
Track patient documentation
Hold marketing until capacity fits
How do you get first customers for mobile IV therapy?
Your first bookings will come from local intent and weekend need, not broad ads. Start with What Is The Cost To Run Hangover IV Treatment Service?, then fill prebooked weekend slots through Google Business Profile, local SEO pages, hotel and concierge referrals, nightlife areas, bachelor and bachelorette events, and wellness partners. Use screening first, keep the language compliant, and watch response time closely, because overbooked nurses become the bottleneck.
First channels
Google Business Profile calls
Local search pages
Hotel concierge referrals
Nightlife and event partners
Capacity guardrails
Year 1 base: 28 clinicians
Modeled capacity: 1,015 treatments/month
Sell weekend windows first
Scale spend after response time holds
How long does it take to start a mobile IV therapy business?
A Hangover IV Treatment Service usually takes 8–16 weeks to start, but the real clock depends on state rules, provider oversight, insurance underwriting, protocol approval, vendor onboarding, hiring, and booking setup. Run these in parallel, not one after another. Don’t set a launch date until compliance and coverage are both confirmed.
Timing drivers
State rules can slow setup.
Medical director contract comes first.
Insurance must be active.
Protocol approval can’t lag.
Launch gates
Supply vendors need onboarding.
Clinicians must be trained.
Booking and dispatch need testing.
Marketing should start early.
Key Takeaways
Compliance comes before bookings, or launch risk rises.
Licensed clinicians set safe capacity and response time.
Inventory and workflow failures can cancel weekend revenue.
Demand should start only after coverage is ready.
State Compliance and Medical Governance
State Compliance and Medical Governance
This is the first gate because mobile IV therapy can’t open on time until the business has verified state law, medical oversight, and a clear scope of practice. If the ordering process, consent forms, charting, or emergency escalation are not approved before launch, you risk delayed bookings and having to stop after the first customer request.
The real bottleneck is opening without legal authority or insurance. Plan for $4,500/month medical director oversight plus about $2,800/month for active malpractice and general liability insurance, then match that to counsel review and licensing checks before marketing turns on.
Lock the legal stack first
Before opening, lock the sequence: counsel review, licensing authority check, provider agreement, protocol signoff, charting standards, and claims review. One clean rule: if the paperwork is late, the launch is late.
Verify scope before scheduling.
Approve consent forms early.
Test emergency escalation steps.
Keep insurance active at launch.
Run one mock chart, one mock consent, and one escalation drill before first revenue. That checks whether the team can document cleanly, respond fast, and stay inside approved protocol on day one.
1
Licensed Clinical Staffing
Licensed Clinical Staffing
The launch gate is simple: you can’t open on time unless licensed clinicians are credentialed, insured, trained, and scheduled for the hours when demand spikes. For this model, the Year 1 mix of 12 registered nurses, 8 paramedics, 2 nurse practitioners, 4 senior flight medics, and 2 lead clinicians only works if weekend coverage, travel rules, and escalation steps are locked before first bookings.
If staffing is thin, the business will either overbook or push cases outside scope, which hurts response time and raises clinical risk. The real readiness signal is not headcount alone; it’s whether each shift can accept bookings, document care, and handle a handoff fast enough to serve peak hangover windows without delays.
Build Coverage Before Sales
Before opening, verify every clinician’s license, insurance, credential file, and protocol training. Then map weekend availability, travel radius, and escalation rules so dispatch knows exactly who can take each call and when a higher-level clinician must step in.
Confirm scope for each role.
Train on IV protocols.
Test peak-hour shift coverage.
Document travel and handoff rules.
Block bookings beyond safe capacity.
Here’s the key test: if a Friday night surge hits, the team must still keep appointments moving without unsafe response times. Weak coverage forces late starts, missed visits, and poor first-day reviews, while tight scheduling supports reliable volume from day one.
2
Supply Vendor and Inventory Readiness
Supply and Stock Readiness
If the first treatment day starts before vendors are lined up, bookings turn into cancellations. This service needs IV fluids, permitted vitamins, catheters, PPE, sharps containers, bags, and pumps or gravity setups on hand, plus storage controls and reorder rules so weekend demand does not break the schedule.
The Year 1 plan assumes 105% medical infusion supplies and IV kits, plus 25% for biohazard waste and sterile logistics. That means the launch depends on vendor contracts, lot tracking, waste pickup, and sterile handling being set before the first booking, or the team may face unsafe substitutions and slower first-day service.
Set Par Levels Before Marketing
Lock in suppliers, delivery timing, and backup sources before ads go live. Set a par level for each item, define reorder points, and document storage rules for fluids and vitamins where permitted. Here’s the quick math: if weekend volume spikes and stock runs short, one missed shipment can block multiple visits.
Assign one person to check lot numbers, expiration dates, and waste pickup dates each week. Test the full restock flow before opening so inventory, not guesswork, drives the schedule. That protects day-one capacity, keeps intake clean, and avoids last-minute patient reschedules caused by sterile supply gaps.
Contract vendors before first booking.
Set par levels by SKU.
Track lot numbers and expiry.
Confirm waste pickup timing.
Keep weekend backup stock.
3
Booking, Dispatch, and Documentation Workflow
Booking, Dispatch, and Records
This workflow is the day-one gate. If online booking, intake forms, payment capture, and HIPAA, the US health privacy rule, records are not live before launch, you can’t safely take paid appointments. The fixed stack starts at $2,150/month for $950 in HIPAA-compliant software plus $1,200 in telehealth maintenance, before fees or travel.
The big risk is not demand; it’s taking bookings you can’t route. With 35% payment processing and merchant fees, plus 60% practitioner travel stipends in Year 1, weak dispatch rules can turn first revenue into refunds, missed visits, and poor patient experience. One clean rule: no live marketing until booking-to-note flow is tested end to end.
Test the full patient path
Before opening, run test bookings from ad click to post-visit note. Verify screening, confirmations, refund rules, no-show policy, dispatch zones, and travel-time rules. If a patient books outside a route window, the system should block or delay the slot, not push the team into a late arrival.
Confirm intake before payment capture.
Set zone and travel-time limits.
Approve refund and no-show rules.
Assign note completion after each visit.
4
Service Menu and Treatment Protocols
Service Menu and Protocol Lock
This launch driver decides whether you can sell safely on day one. The menu has to match approved protocols, so each package should spell out what is included, what is not, and which claims staff can say. If the offer is vague, booking slows and clinicians start improvising, which is a real opening risk.
Here’s the quick math: Year 1 prices run from $180 for paramedic-supported services to $450 for lead clinician services. That only works if the price ladder matches scope, screening rules, contraindications, and escalation steps. Weak protocol control can trigger refunds, charting gaps, or services beyond scope, all of which can delay launch.
Set the Menu Before Booking Goes Live
Lock the launch pack before the first ad runs: package contents, allowed add-ons, vitamin rules where permitted, consent language, documentation templates, and refund policy. Use plain patient-facing language that avoids cure promises, and keep the wording aligned with what the clinician can actually do. That keeps sales, care, and compliance on the same page.
Test the flow end to end with one completed chart, one screening failure, and one escalation case before opening. If intake, consent, or follow-up notes are unclear, first-day appointments can stall and staff may pause bookings. The fix is simple: assign one owner to approve every protocol version, price change, and menu edit before launch.
Define inclusions and exclusions first
Write claims that match protocol
Map screening and escalation rules
Train staff on refund triggers
5
Local Demand and First Bookings
Local Demand You Can Cover
Local search visibility matters because this service wins on fast, nearby bookings, not broad awareness. If weekend availability is live but search, reviews, and referral paths are weak, demand stays thin; if marketing works too soon, inquiries can arrive before staff coverage. The launch signal is simple: local search, hotel, concierge, nightlife, and event traffic must match open slots.
Plan around the stated $5,500/month digital marketing and SEO management spend. That budget should support Google Business Profile, local SEO, paid local search, hospitality outreach, and event targeting, with fast reply times for booking requests. One clean rule: don’t turn on demand you can’t serve.
Prebook the Weekend, Then Open Ads
Before launch, verify the booking path, response time, and weekend roster are all aligned. Build the first week around hotels, concierge desks, bachelor and bachelorette events, nightlife areas, and wellness partners, then test that every lead can reach a real booking channel fast. Reviews and partner referrals should be in place before paid traffic scales.