How Much It Costs To Start A Hangover IV Treatment Service: $857K
You’re funding a mobile Hangover IV Treatment Service before demand is proven, so the key number is total cash need, not just equipment This first-year planning model shows $857K minimum cash, $198K in setup assets and opening inventory, and Month 1 breakeven under the stated volume assumptions These ranges are planning assumptions, not vendor quotes or legal, tax, or medical licensing advice
Estimate Startup Costs with Calculator
Startup CAPEX Calculator
Estimates capitalized startup assets only for launch setup; it does not include inventory, payroll runway, or other operating cash needs.
!
Scope note This calculator covers capitalized launch assets only. It excludes the $25,000 initial inventory stockpile, consumable IV bags, vitamins, medications, licensing, insurance premiums, payroll, marketing, working capital, debt service, and deposits.
Calculate Fuding Needs
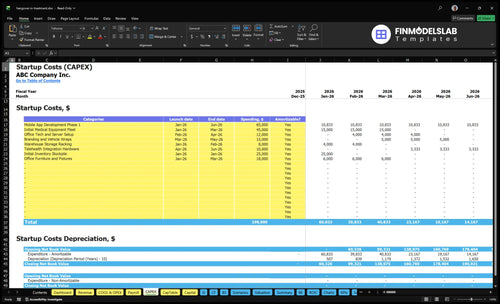
Startup cost summary
This table breaks out startup asset costs and excluded launch cash needs for a mobile hangover IV treatment service.
Highlighted CAPEX$198,000Base planning example
Excluded cash needs$857,000Outside CAPEX total
Funding need$1,055,000CAPEX + excluded cash needs
Cost Category
Base Estimate
Main Cost Driver
CAPEX Calculator
Mobile app and telehealth setup
$87,000
App build, telehealth hardware, and booking tools
Yes
Initial medical equipment fleet
$45,000
Clinical equipment for mobile IV treatments
Yes
Office furniture and storage setup
$26,000
Warehouse racking, furniture, and fixtures
Yes
Branding and vehicle wraps
$15,000
Vehicle wraps and launch branding
Yes
Opening inventory stockpile
$25,000
Initial IV supplies, vitamins, and stock
Yes
Payroll runway and operating reserve
$857,000
Fixed overhead, Year 1 admin payroll, and launch runway
Startup cost moves fast here because clinician coverage, inventory, dispatch tech, and marketing scale together. Lean stays cash-light, base matches the model, and full needs more working capital for wider reach.
Lean, base, and full launch paths show how cash need changes with scope.
Scenario
Lean Launchcash-light
Base Launchmodeled base
Full Launchexpansion-ready
Launch model
Single-provider launch in one small service area with manual booking and deferred app work.
One-market launch using the modeled clinician mix, app support, and centralized dispatch.
Expanded launch across a wider service radius with more staff, more inventory, and heavier marketing.
Typical setup
One clinician covers a tight radius, with manual scheduling and a smaller stock pile.
A 28-clinician Year 1 setup uses app-based dispatch, core inventory, and one central ops team.
Coverage widens, inventory rises, and the back office needs more staff and working capital.
Cost drivers
Deferred app build
smaller service area
manual dispatch
lighter inventory
lower marketing
App build
28 Year 1 clinicians
opening inventory
central office overhead
standard marketing
Wider service radius
more clinicians
more inventory
more equipment
stronger marketing
Planning rangeCAPEX only
$350,000 - $650,000Lower cash band
$857,000 - $1,100,000Model anchor
$1,200,000 - $1,700,000Expansion band
Best fit
Founders testing demand in one zone with limited cash.
Teams that want to match the modeled plan and scale inside one market.
Operators ready to fund broader coverage, heavier marketing, and more staff.
!
Planning note: Scenario ranges are researched planning assumptions, not exact vendor quotes or financing offers.
How much funding should a hangover IV treatment service raise?
A Hangover IV Treatment Service should raise at least $857K in cash, not a shopping-list budget, if it wants a real launch runway. Use that raise to prove Month 1 breakeven and a 1-month payback on paper, then stress test slower onboarding, lower utilization, and delayed reimbursement. With 28 clinicians split across 12 registered nurses, 8 paramedics, 2 nurse practitioners, 4 senior flight medics, and 2 lead clinicians, Year 1 revenue comes down to treatment volume times $180 to $450 pricing under 200% to 350% capacity assumptions.
Cash need
$857K minimum cash
Month 1 breakeven target
1-month payback goal
Buffer for onboarding delays
Model tests
28 clinicians in Year 1
$180 to $450 treatment prices
200% to 350% capacity assumptions
Stress reimbursement timing
What hidden costs should you plan for when starting a hangover IV treatment service?
Plan for more than the $45K equipment fleet. For a Hangover IV Treatment Service, the biggest hidden costs are the What Is The Cost To Run Hangover IV Treatment Service? items you pay every month: $28K for malpractice and general liability insurance, $45K for a medical director retainer, plus payment processing at 35% of Year 1 revenue, travel stipends at 60%, and biohazard waste at 25%. The $45K fleet does not cover consumable supplies, vitamins, medications, launch marketing, or working capital.
Monthly burn items
$28K insurance cost
$45K medical director retainer
35% payment processing
60% travel stipends
Pre-open costs
Healthcare attorney review
State scope-of-practice checks
Clinician onboarding and credentialing
Training, fuel, and expired inventory
What are the biggest startup costs for a hangover IV treatment service?
The biggest startup cost for a Hangover IV Treatment Service is not one single line item; it shifts by founder profile and state rules. On launch, the biggest cash needs can be $65K for app development, $45K for medical equipment, and $25K for inventory, plus monthly pressure from $45K medical director oversight, $28K insurance, $55K digital marketing, and about $258K per month in Year 1 admin wages.
Launch costs
$65K mobile app development
$45K equipment fleet
$25K inventory stockpile
$18K office setup
Monthly pressure
$45K medical director oversight
$28K insurance coverage
$55K digital marketing
$258K Year 1 admin wages
A licensed clinical founder may cut hiring friction, but it does not remove compliance, malpractice, or medical oversight planning. Add $15K for branding and vehicle wraps and $12K for office tech and servers, so the real startup load is spread across setup, regulation, and demand generation.
Key Takeaways
Licensure and oversight costs start before launch.
Durable gear and inventory need separate budgets.
Insurance and compliance costs are recurring and state-driven.
Staffing, software, and processing fees scale with revenue.
Hangover IV Treatment Service Core Five Startup Costs
Licensing, Compliance, And Medical Oversight Startup Expense
Licensing and Oversight
This line covers business formation, healthcare attorney review, state scope-of-practice checks, medical protocols, standing orders where allowed, provider agreements, and local permits. The recurring anchor is $45K per month for medical director oversight, or $540K per year before growth. Budget it as a core fixed cost, not a one-time setup item.
Estimate Inputs
Start with the number of states, the number of service lines, and the provider model. Here’s the quick math: 1 state x 1 protocol set x 1 medical director arrangement is cheaper than a multi-state build. Use quotes for attorney review, permit fees, and oversight contracts, then add months of coverage before launch.
Count states first.
Price each protocol review.
Cover launch months upfront.
Control the Spend
Keep the first launch narrow so the attorney and medical director work is reused, not rebuilt. Don’t spread into new states before the scope-of-practice matrix is signed off. The Compliance and Quality Officer starts in Month 13 at $75K annual salary, so someone still has to own compliance work before then.
Launch in one state first.
Reuse one protocol library.
Assign pre-launch ownership now.
Scope-of-Practice
State rules decide whether nurses, paramedics, nurse practitioners, or supervising clinicians can do each service. That changes staffing, supervision, and who signs orders. Build a state-by-state matrix before launch, because the same IV workflow can be allowed in one state and restricted in another.
Pre-Launch Roles
Before the Month 13 hire, assign compliance to a founder or operator and document every protocol, permit, and provider approval. The $75K compliance role is only $6,250 per month on an annualized basis, while the oversight fee stays at $45K per month, so the internal seat does not replace external medical governance.
Insurance And Risk Management Startup Expense
Cover Everything
Insurance is not optional for a mobile IV service. Build for professional liability, malpractice, general liability, commercial auto, workers’ compensation, and cyber and privacy coverage. The researched monthly malpractice and general liability anchor is $28K, but quotes still move with state, clinician mix, claims history, travel radius, and whether you use medicines beyond hydration and vitamins.
What It Pays For
Budget for policy deposits, certificates of insurance for landlords and partners, and any required endorsements. Here’s the quick math: estimate months of coverage × quoted premium, then add deposit and admin fees. What this estimate hides is the spread across states and the jump in price when services expand beyond simple hydration or when clinician credentialing changes the risk class.
Get state-by-state quotes.
Price the full service menu.
Match coverage to travel radius.
Cut Risk, Not Coverage
Lock scope first, then shop quotes, because underwriters price what you actually do. Keep the medication menu tight, enforce clinician credentialing, and avoid adding travel miles unless the revenue supports the premium jump. To be fair, savings come from clean files and narrow risk, not from skimping on coverage.
Review claims history early.
Track every service area.
Renew certificates before launch.
HIPAA Risk
Because care happens in homes, offices, and hotels, privacy risk is real. Tie insurance planning to the Health Insurance Portability and Accountability Act (HIPAA), mobile charting, device security, and incident response. Partner and landlord demands for certificates can also slow launch, so get those forms ready before the first booking.
IV Supplies, Vitamins, And Opening Inventory Startup Expense
Opening Stock
Treat the first buy as working capital, not durable CAPEX, unless your accounting policy says otherwise. The researched opening inventory stockpile is $25K and should cover saline or hydration fluids, tubing, catheters, PPE, vitamins, permitted anti-nausea add-ons, bandages, disinfectants, sharps disposal, and sterile logistics.
Price The Stock
Build the estimate from units × unit price, supplier quotes, and weeks of coverage by treatment mix. The key inputs are how many IV kits you expect to use, how fast each item expires, and what it costs to store and move waste. The $25K opening buy sits inside launch cash, not long-term asset spend.
Count kits by service mix.
Price each item by quote.
Add waste pickup quotes.
Control Waste
Keep the reorder plan tied to treatment mix, expiration dates, weekend demand, and service radius. That is where inventory gets lost: too much stock for slow routes, not enough for peak nights, or expired product sitting in the van. Tight buy schedules usually save more than bulk buys, without hurting speed or compliance.
Reorder by route volume.
Track expiring items weekly.
Stock weekends separately.
Watch The Drag
Year 1 medical infusion supplies and IV kits run 105% of revenue, and biohazard waste plus sterile logistics run 25%. So the inventory line is not small: every extra kit and every long pickup route hits cash fast. If you do not turn stock quickly, the first problem is waste, not shortage.
Mobile Setup And Durable Clinical Equipment Startup Expense
Setup Cost
This line covers durable gear only, not IV fluids or meds. The researched setup budget totals $108K: $45K medical equipment fleet, $15K branding and vehicle wraps, $8K warehouse racking, $12K office tech and server setup, $10K telehealth hardware, and $18K furniture and fixtures.
What It Covers
Use this budget for portable treatment gear, vital-sign monitors, coolers or refrigeration, sanitation tools, sharps containers, clinical bags, tablets, payment devices, and backup kit. Price it with vendor quotes by unit count, then check whether each item is durable, serviceable, and field-ready. One clean rule: don’t mix it with opening inventory.
Quote each unit separately
Keep disposables in inventory
Test battery life and transport
Trim Waste
Cut setup spend by buying only the fleet needed for launch, standardizing tablet and payment hardware, and using modular storage instead of custom build-outs. Watch the wrap line: the $15K branding and vehicle-wrap amount does not include any vehicle purchase. Buy-versus-lease should be a separate input, not assumed.
Lease if route volume is unclear
Skip custom cabinet work
Use one hardware standard
Field Backup
A lean launch still needs one backup set for monitors, tablets, payment devices, sanitation, and sharps handling. If a unit fails on the road, replacement speed matters more than polish, so keep redundancy inside the $45K equipment fleet instead of pushing it into supplies or office tech.
Staffing, Booking, And Launch Operations Startup Expense
Launch payroll
Keep pre-opening work separate from ongoing payroll. This launch line covers recruiting, credential checks, onboarding, training, scheduling setup, and dispatch readiness, plus the booking stack and telehealth tools. The named admin team alone starts at $310K a year: $95K + $45K + $45K + $55K + $70K.
Clinical base
The clinical staffing model uses 12 registered nurses, 8 paramedics, 2 nurse practitioners, 4 senior flight medics, and 2 lead clinicians. To estimate payroll, multiply each headcount by its annual pay and add benefits and shift coverage. No role pay rates were provided, so the current model gives count, not total clinical burn.
Booking stack
To trim launch waste, hire in waves and keep one scheduling process until volume is proven. The fixed booking layer is $950 per month for Health Insurance Portability and Accountability Act-aware software plus $12K per month for telehealth maintenance, so the base tech run rate is $12,950 before payment fees. Payment processing adds 35% of revenue.
Dispatch gate
Use the launch budget to lock the compliance chain, not just the staff list. State-by-state rules decide whether nurses, paramedics, nurse practitioners, or supervising clinicians can deliver service, so credentialing and scope checks sit ahead of booking. If dispatch is ready but coverage rules are not, you can’t take the order.