 Time to Open6-12 monthsOpening prep
Time to Open6-12 monthsOpening prepHow To Open A Primary Care Clinic In 6–12 Months With Clean Claims

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open6-12 monthsOpening prep  Launch Sequence7 stagesCompliance first
Launch Sequence7 stagesCompliance first Key BottleneckCredentialing gatePayer lead time
Key BottleneckCredentialing gatePayer lead time First Revenue StepBilled visitsClaims live
First Revenue StepBilled visitsClaims live


You’re building a clinic before the first patient walks in, so the launch plan must line up licensing, payer setup, staffing, facility readiness, EHR, billing, and demand This guide uses a 6–12 month US launch window and a 5-year operating model with Year 1 staffing of 2 GPs, 1 nurse practitioner, and 1 physician assistant Use the model to test timing, capacity, and cash runway before you sign fixed commitments
Time to Open6-12 monthsOpening prepLaunch Sequence7 stagesCompliance firstKey BottleneckCredentialing gatePayer lead timeFirst Revenue StepBilled visitsClaims liveLaunch timeline
Short web summary of the clinic launch plan; the XLSX export holds the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10
Legal and licensing
- Form entity
- Register tax IDs
- File permits
- Final compliance
Facility and buildout
- Lease space
- Renovation work
- Install furnishings
- Security install
- Final walkthrough
Payer and billing
- Payer mapping
- Provider enrollment
- Credential packet
- Credential follow-up
- Claim testing
Staffing and training
- Hire manager
- Recruit clinicians
- Hire support staff
- Background checks
- Train workflows
EHR and IT
- Choose EHR
- Setup hardware
- Build templates
- User testing
- Billing go-live
Vendors and launch ops
- Order supplies
- Set lab vendors
- Launch outreach
- Open scheduling
- Opening week
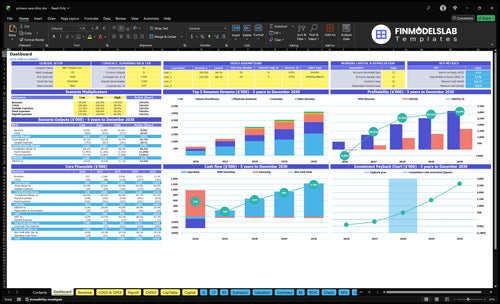
Want to test the clinic launch plan against the numbers?
It shows revenue, costs, cash needs, assumptions, and break-even logic, so open the Primary Care Clinic Financial Model Template.
Financial model highlights
- 2 GPs, 1 NP, 1 PA
- $52.6k monthly revenue
- 160% variable cost load
- $20.1k fixed operating costs
- Ramp, utilization, cash gap
How long does it take to open a primary care clinic?
A Primary Care Clinic usually takes 6–12 months to open in the US. Start with entity formation and licensing, then site selection, payer credentialing, buildout, EHR setup, hiring, vendor setup, marketing, and opening-week testing. The biggest delays are payer credentialing, facility buildout, EHR implementation, provider hiring, inspections, and incomplete paperwork, so don’t set an opening date until payer effective dates, staff schedules, and billing tests are real.
Typical opening sequence
- Form entity and get licensed
- Pick site and negotiate lease
- Start payer credentialing early
- Set up EHR and hire staff
Delays that move launch
- Payer approval can lag
- Buildout can slip on permits
- EHR setup can take longer
- Testing can fail on missing docs
How do you get patients for a new primary care clinic?
You get patients for a Primary Care Clinic before opening: claim insurance directory listings, set up a Google Business Profile, build local SEO, turn on online scheduling, and start employer outreach, referral relationships, community groups, and review-building workflows; keep eligibility checks, copay collection, and clean claims tied to every booked new-patient visit, and see What Is The Estimated Cost To Open And Launch Your Primary Care Clinic? for the launch budget side. Year 1 patient acquisition marketing is modeled at 30% of revenue, and the clinic needs about 390 monthly visits across GP, nurse practitioner, and physician assistant capacity.
Before opening
- Claim insurance directory listings
- Set up Google Business Profile
- Publish local SEO pages
- Open online scheduling
After inquiry
- Reach out to employers
- Build referral relationships
- Collect copays at check-in
- Submit clean claims fast
What do you need to open a primary care clinic?
To open a Primary Care Clinic, you need legal clearance, licensed providers, payer enrollment, compliant operations, and a working billing setup before the first visit. Start with entity formation, ownership review, a 10-digit National Provider Identifier, malpractice coverage, and clean-claim readiness; then track performance with What Is The Most Important Indicator To Measure The Success Of Your Primary Care Clinic?.
Launch Requirements
- Form the legal entity
- Review state ownership rules
- Verify provider licenses
- Get NPI and payer enrollment
Operating Readiness
- Set HIPAA privacy policies
- Build OSHA safety procedures
- Add EHR and billing workflows
- Confirm CLIA-waived testing needs
Build the primary care clinic opening checklist
Launch readiness checklist
Use this go-live approval checklist to confirm the clinic is ready before opening.
Licensing
- Ownership rules and entity filedCritical
This confirms the clinic can open under the right legal structure.
- Provider licenses and NPI activeCritical
Licensed providers and a National Provider Identifier are needed before patient care starts.
- Malpractice coverage boundCritical
Coverage should be active before the first visit and staff duty starts.
- HIPAA and OSHA policies readyHigh
Privacy and safety rules must be in place before patient data and clinic work begin.
Facility
- Lease and buildout signedCritical
The space must be secured and ready for clinical use before opening.
- Accessibility and exam rooms clearedHigh
Patients and staff need usable rooms, clear paths, and proper access.
- Medical waste pickup activeHigh
Waste handling must be live before the clinic sees its first patient.
- CLIA waived testing approvedMedium
This is only needed if the clinic will offer waived lab testing at launch.
Systems
- EHR configured and testedCritical
The EHR must support charting, orders, and patient records on day one.
- Billing workflow test completedCritical
A clean billing test shows claims can move from visit to payment.
- Eligibility checks connectedHigh
Coverage checks help avoid denials and bad balances from the first week.
Staffing
- Providers hired and scheduledCritical
The provider roster must match opening demand and service hours.
- Front desk and MA coverageCritical
Front desk and medical assistant coverage keep intake and rooms moving.
- Intake and consent training doneHigh
Staff need one clear process for check-in, consent, and handoffs.
Revenue
- Payer contracts effectiveCritical
Visits cannot cash flow well if payer contracts are not live.
- Claim submission test passedCritical
This is the fastest check that claims can be sent and received.
- Patient visit schedule bookedHigh
Opening without booked visits turns fixed costs into a cash burn.
Signoff
- Cash runway covers Month 13Critical
The model shows minimum cash at Month 13, so runway needs to hold through then.
- Opening-week schedule approvedHigh
A clear first-week plan cuts no-shows, gaps, and missed handoffs.
- Launch assumptions reviewedHigh
Capacity, pricing, and staffing should match the forecast before go-live.
- Go-live signoff approvedCritical
This is the final gate before the clinic opens to patients.
Want the six launch drivers that decide opening readiness?
1Payer Enrollment
GateKeeps first visits payable by activating provider and payer status before opening.
2Facility Readiness
Day 1Clears exam rooms, waste, and privacy checks so day-one care starts without inspection delays.
3EHR & Billing
Clean claimsTurns bookings into clean claims by testing intake, coding, and submission before launch.
4Hiring
4 providersBuilds the Year 1 team of four providers and support staff for stable coverage.
5Pre-Opening Marketing
Full booksFills the first month schedule using directory listings, referrals, and local search before opening.
6Ramp Validation
$52.6K/moChecks utilization, reimbursement lag, and fixed costs so the opening plan matches cash needs.
Payer Credentialing And Provider Enrollment
Payer Credentialing
If the clinic opens before payer credentialing is live, booked visits can turn into held claims instead of cash. This gate sits before first clean claims, so it is a launch blocker, not a back-office task. The clinic needs the National Provider Identifier, taxonomy, CAQH profile, commercial applications, Medicare enrollment, Medicaid enrollment where needed, plus active contracts, fee schedules, and effective dates.
The risk is opening with demand but no reimbursable panels. You can still see patients, but billing may stall, cash collections slow, and staff spend more time fixing claims than serving patients. One clean visit on paper is not enough; the payer record has to be active before the first scheduled appointment that is meant to bill insurance.
Track Payer Dates
Build a payer tracker before opening and assign one owner to keep it current. Record NPI, taxonomy, CAQH status, application date, contract status, fee schedule receipt, and effective date for each payer so scheduling, billing, and front desk teams know which visits are reimbursable on day one.
Test one mock claim per payer before launch. If a commercial plan, Medicare, or Medicaid file is still pending, delay insurance-based scheduling for that panel or mark it clearly as self-pay until the credentialing path is active. That keeps opening day aligned with real cash flow, not just patient demand.
1
Facility And Compliance Readiness
Facility Readiness
If the clinic space is not fully set up, opening slips fast. Exam rooms, accessibility, infection control, sharps and medical waste handling, privacy, OSHA procedures, cleaning, storage, signage, and inspection readiness all have to be in place before the first patient walks in.
Here’s the quick math: fixed facility costs are $12,000 rent, $1,500 utilities, $1,000 cleaning, and $500 office supplies, or $15,000 per month before staffing and medical supplies. If any required approval is missing, you can still carry the full burn while waiting to open.
Verify Before You Set the Open Date
Check state, local, landlord, and medical board rules before signing off on the launch date. Decide early whether to offer CLIA-waived testing, because that choice changes the room setup, procedures, and verification steps. What this estimate hides is the time lost when one missing item blocks inspections or move-in.
- Confirm exam room layout and accessibility
- Set sharps and waste pickup process
- Document cleaning and OSHA steps
- Install privacy, storage, and signage
- Test supplies before first patient day
Assign one owner to the readiness checklist and one to inspection files. If the clinic passes paper review but fails on cleaning logs, waste handling, or room setup, day-one care gets delayed and the team starts with avoidable risk.
2
EHR, Billing, Scheduling, And Claims Workflow
Day-One EHR Workflow
If the clinic cannot move a visit from booking to a clean claim, opening day turns into rework. This setup has to cover scheduling, online booking, intake, eligibility, copays, coding, superbills, clearinghouse submission, patient portal, denial management, and reporting before the first patient walks in.
The cash impact is real: fixed EHR software fees are $1,800/month, and billing and collections fees are modeled at 50% of Year 1 revenue. So a broken workflow can hit both service speed and cash needs right away.
Test the Full Claim Path
Run a mock visit end to end before opening. Verify these inputs: visit type, payer plan, eligibility check, copay collection, diagnosis and procedure coding, superbill creation, claim scrub, clearinghouse send, portal message, and denial follow-up. One clean test beats fixing ten failed first claims.
- Confirm booking and intake fields.
- Check payer eligibility rules.
- Test copay and claim submission.
- Review denial and reporting screens.
If staff learn the workflow after launch, first appointments can stall at coding or submission, which slows cash and frustrates patients. A tested setup helps the clinic start with clean claims, not backlog.
3
Provider And Staff Hiring
Staffing For Day-One Coverage
Opening a primary care clinic is mostly a staffing problem. The Year 1 model needs 2 GPs, 1 nurse practitioner, and 1 physician assistant, plus 1 clinic manager at $85,000/year and 1 front desk coordinator at $40,000/year. If any role is late, schedules shrink, visits stack up, and day-one access breaks before revenue starts.
The bigger risk is supervision and handoff gaps. By Year 5, the plan grows to 5 GPs, 3 nurse practitioners, 2 physician assistants, 1 dietitian, and 1 counselor. That means scope, coverage, and backfill rules must be set before opening, or patient service failures rise fast when a provider is out.
Hire To Match The First Schedule
Build the team backward from the opening calendar. Lock provider start dates first, then confirm schedules, scope, supervision, SOP training, front desk scripts, billing handoffs, and coverage plans. The clinic manager should own daily staffing, and the front desk coordinator should handle booking, intake, and overflow. Test one full clinic day before launch.
- Match shifts to booked visits.
- Document sick-day coverage.
- Train on billing handoffs.
- Run a full mock day.
If onboarding slips by even a week, the clinic can open with empty slots, weak call coverage, and slower check-in. That hurts patient trust fast. A clean start needs a staffed front desk, clear provider escalation paths, and enough clinical coverage to absorb no-shows, add-ons, and same-day care.
4
Pre-Opening Patient Acquisition
Pre-Opening Patient Demand
Patients won’t fill the first schedule unless demand is built before opening. For a primary care clinic, that means live insurance directory listings, a working Google Business Profile, local SEO, referral partners, employer outreach, and community outreach so the first visit slots have real buyers, not just interest.
Year 1 marketing is modeled at 30% of revenue, so this is a launch cost, not a side task. Here’s the quick math: a weak pre-open pipeline leaves the clinic paying staff and software while the calendar stays light, which slows cash and pushes the team away from 600% GP capacity and 550% NP/PA capacity.
Book Visits Before Day One
Build the launch plan around booked visits, show rates, eligibility success, and completed claims, not clicks. The clinic should test online scheduling, intake, and referral follow-up before opening so the front desk can turn interest into real appointments without delay.
- Activate directory listings early.
- Test online booking end to end.
- Assign referral and employer outreach.
- Set review requests after visits.
If insurance data or scheduling links are slow, the first month will need rework instead of revenue. One clean rule: if a patient can’t find, book, and confirm the visit fast, the clinic is not launch-ready yet.
5
Operating Model And Financial Ramp Validation
Ramp Validation
Opening only works if the visit ramp is real, not just hopeful. The model uses $52,560/month in Year 1 revenue from 2 GPs at 160 monthly visits each and 1 NP plus 1 PA at 180 monthly visits each, with visit prices of $150 and $120. That makes provider utilization the first cash test.
If visit mix, payer mix, or reimbursement lag slips, you can still open on paper but miss the cash needed for rent, wages, and software. The known fixed base is about $16,800/month before provider pay and billing costs, so weak ramp math can push breakeven out fast and strain runway in month one.
Pre-Open Cash Check
Build the launch plan around the first 90 days of visits, collections, and staffing. Check whether each provider can actually hit the modeled schedule, then test the visit types, payer mix, and claim lag against the opening date so you know when cash starts moving.
- Match staffing to opening week volume.
- Track clean claims after first visits.
- Stress test rent and wage timing.
- Confirm runway against fixed costs.
Run one simple test: can the clinic absorb delayed payments and still cover $12,000 rent, $1,500 utilities, $1,000 cleaning, $500 supplies, and $1,800 software? If not, trim the opening schedule before the lease, payroll, and billing clock start.
6
Related Products
- Primary Care Clinic Porter's Five Forces Analysis
- Primary Care Clinic BCG Matrix
- Primary Care Clinic Business Model Canvas
- 7 Critical Financial KPIs for Primary Care Clinic Growth
- Primary Care Clinic Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Primary Care Clinic Profit Margins
- How Much Does It Cost To Run A Primary Care Clinic Monthly?
- Primary Care Clinic Startup Costs: $345K CAPEX And $558K Cash
- Primary Care Clinic Financial Model Template in Excel
- How Much Does a Primary Care Clinic Owner Make? 5-Year View
- How to Write a Business Plan for a Primary Care Clinic
- Primary Care Clinic Marketing Mix
- Primary Care Clinic Marketing Plan
- Primary Care Clinic Business Proposal
- Primary Care Clinic PESTEL Analysis
- Primary Care Clinic Pitch Deck Example Editable PPTX
- Primary Care Clinic Business SWOT Analysis
- Primary Care Clinic Value Proposition Canvas
Frequently Asked Questions
Start with ownership review, entity formation, provider licensing, National Provider Identifier setup, and payer credentialing Then secure the site, EHR, billing workflow, malpractice coverage, and staff A practical US launch window is 6–12 months The researched Year 1 model starts with 2 GPs, 1 nurse practitioner, and 1 physician assistant