 Owner incomeNear $0
Owner incomeNear $0How Much Does a Primary Care Clinic Owner Make? 5-Year View

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner incomeNear $0  Net margin-22% to 345%
Net margin-22% to 345% Revenue for target pay$1.19M
Revenue for target pay$1.19M Business difficultyHard
Business difficultyHard


Key Takeaways
- More visits raise revenue only when capacity stays safe.
- Mix and reimbursement drive income even at flat volume.
- Fixed overhead and staffing set the break-even floor.
- No-shows and collections issues weaken cash from each visit.
Owner incomeNear $0Net margin-22% to 345%Revenue for target pay$1.19MBusiness difficultyHardWant to test your clinic owner income?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
Want to check your Primary Care Clinic owner income path?
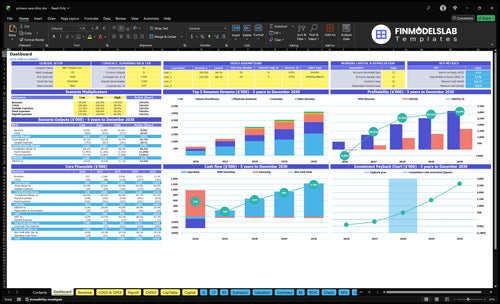
The Primary Care Clinic Financial Model Template shows revenue, margin, costs, reserves, and owner take-home in one view. It also includes dashboard, revenue build, provider capacity, payer mix assumptions, COGS, variable expenses, fixed overhead, staffing, cash flow, and owner pay outputs; charts move from $630,720 in year 1 to $1,185,615 in year 2, with operating profit rising from -$13,895 to $409,073 before provider compensation and reserves. Open the model.
Owner-income model highlights
- Owner take-home plus reserves
- Revenue build and payer mix
- Test staffing and capacity
How does payer mix affect primary care clinic profit?
For a Primary Care Clinic, payer mix can swing profit even when visit count stays flat; if you're also sizing startup spend, see What Is The Estimated Cost To Open And Launch Your Primary Care Clinic? Same visits, different payers, different cash. Here’s the quick math: first-year pricing uses $150 for GP visits and $120 for NP and PA visits, while billing and collections fees run at 50% of revenue, so denials, copays, patient responsibility, commercial contracts, Medicare, Medicaid, and self-pay all change net collections.
Cash per visit
- $150 GP visit price
- $120 NP visit price
- $120 PA visit price
- Reimbursement drives owner income
Collection risk
- 50% first-year billing and collections fees
- Denials cut net cash
- Copays change collections speed
- Contracts vary by payer
How much can a primary care clinic owner take home after expenses?
A Primary Care Clinic owner may take home $0 in year one in this case because operating profit is -$13,895 before provider pay, debt, reserves, taxes, and distributions; see What Is The Most Important Indicator To Measure The Success Of Your Primary Care Clinic? for the KPI lens. Year two improves to $409,073 before those same exclusions, but owner income still depends on provider payroll and cash needs.
Year 1 math
- Revenue: $630,720
- COGS: $50,458
- Variable costs: $50,458
- Overhead plus support wages: $543,700
Owner pay risk
- Operating profit: -$13,895
- Year 2 profit: $409,073
- Provider payroll lowers take-home
- Visits, reimbursement, or capacity must rise
Is a primary care clinic more profitable if the owner sees patients?
Yes — in a Primary Care Clinic, the owner seeing patients usually helps early cash flow because it replaces some provider payroll. In the first-year model, 2 GPs, 1 Nurse Practitioner, and 1 Physician Assistant produce 390 visits/month at 550% to 600% capacity, so owner-clinical work can lift billable output fast. The tradeoff is simple: more clinical time can mean less time for management, and burnout risk goes up if the owner works full time.
Owner sees patients
- Replaces some provider payroll.
- Improves early cash flow.
- Raises billable capacity.
- Can increase burnout risk.
Owner steps back
- Part-time clinician-manager keeps control.
- Multi-provider scale needs payroll leverage.
- Scheduling must stay tight.
- Revenue cycle controls must stay strong.
Want to see what really drives clinic owner income?
1
390/moVisit Volume
Year 1 runs at 390 visits a month, so even small booking gains push revenue past the $630.7K base.
2
$120-$170Payer Mix
Core visit prices range from $120 to $170, and a heavier share of higher-paid GP visits lifts take-home fast.
3
$302.5KStaffing Model
Support wages reach $302.5K in year 1, and the model still shows a -22% operating margin before provider pay.
4
$20.1K/moOperating Overhead
Rent, utilities, insurance, EHR, cleaning, office, and professional fees total $20.1K a month, so fixed cost control drives break-even.
5
$100-$135Service Mix
Dietitian and counselor visits begin in year 3 at $100 to $135, which adds revenue but usually at a lower ticket than core care.
6
4.5%-5.0%Revenue Cycle
Billing and collections fees stay in the 4.5% to 5.0% range, so tighter claims work keeps more cash in the clinic.
Primary Care Clinic Core Six Income Drivers
Visit Volume And Provider Productivity
Visit Volume
More completed visits drive net patient revenue because this clinic bills fee for service. The model starts at 390 visits/month in year one, then reaches 707 visits/month in year two as provider count and capacity rise. One line says it best: if the schedule fills, income rises.
The catch is capacity. Volume only helps if access and care quality stay steady. If visits get rushed, no-shows rise, or staff get overloaded, the owner can lose repeat business and cash conversion. Once fixed overhead is covered, extra visits add more to take-home income and less to survival.
Protect the Schedule
Track completed visits, booked visits, no-show rate, and visits per provider role each week. Here’s the quick math: compare planned capacity to actual visits, then check where slots are leaking. That tells the owner whether growth is real revenue or just a crowded calendar.
- Completed visits per month
- No-show rate by provider
- Visits per clinician session
- Late-cancel and open-slot rate
Use the targets already in the model, from 390 to 707 visits/month, and add capacity only when providers can still give safe, timely care. If schedules tighten too far, owner profit can fall even while top-line revenue rises.
1
Payer Mix And Net Reimbursement
Payer Mix And Net Reimbursement
Same visit count can still produce very different owner income. At the first-year assumptions, a GP visit prices at $150 and an NP or PA visit at $120, then billing and collections take 50% of revenue; by the mature year, pricing rises to $170, $140, and $140, with fees down to 45%. Payer mix matters because commercial, Medicare, Medicaid, self-pay, denials, and patient balances change what the clinic actually keeps.
Here’s the quick math: if 10 visits shift from NP or PA pricing to GP pricing, gross charges rise by $300 at first-year rates, and net cash rises by about $150 after billing and collections. That’s why reimbursement per visit can lift take-home pay even when visit volume stays flat. What this estimate hides: contract rates, denials, and slow patient collections can erase a lot of that gain.
Track Net by Payer, Not Just Visits
Build the forecast by payer and provider type, not one blended rate. Track allowed amount, collection rate, denial rate, and patient balance collection each month, then compare them with the assumed 50% first-year fee load and 45% mature-year load. If reimbursement falls below plan, owner pay drops fast even when the schedule stays full.
Test which mix gives the best net yield after fees: commercial, Medicare, Medicaid, and self-pay. A small shift toward better-paid visits can improve cash flow without adding staff or room capacity. Keep payer contracts, copays, and write-off rules tight, because weak collections turn good volume into weak profit.
- Track net revenue per visit.
- Separate by payer and provider.
- Watch denials and patient balances.
- Reprice when contracts reset.
2
Provider And Clinical Staffing Model
Provider and Clinical Staffing
This staffing model turns providers into capacity and support staff into throughput protection. Year 1 uses 2 GPs, 1 Nurse Practitioner, 1 Physician Assistant, plus clinical and admin support, with disclosed support wages of $302,500. Provider payroll is not included, so owner income is overstated unless employee or contractor pay is added in.
Here’s the quick math: more visits only help if the team can book, room, code, and bill them. If staffing is thin, no-shows, slow check-in, claim errors, and rework cut cash flow and margin. One line says it all: headcount without throughput does not pay the owner.
Measure Labor Against Visits
Track visits per provider, rooming time, claim lag, denial rate, and days in A/R every week. The clinic manager, front desk coordinator, and medical biller should be judged on schedule fill, copay collection, and clean claims, because those jobs protect revenue that already hit the schedule. If those metrics slip, owner pay slips too.
Before paying yourself, model provider compensation explicitly. If doctors or advanced practice clinicians are employees or contractors, their pay comes out of profit. Test staffing against volume: if added labor does not raise completed visits and collections, it compresses margin instead of creating income.
3
Fixed And Operating Overhead
Fixed And Operating Overhead
$20,100/month in fixed overhead is the break-even hill the clinic must clear before the owner gets paid. That includes $12,000 rent, $1,500 utilities, $2,500 insurance, $1,800 EHR software, $1,000 cleaning, $500 supplies, and $800 professional services. These costs stay put when visits slow, so low volume hits owner income fast. Annual fixed overhead is $241,200.
The owner only starts to feel real upside after volume covers this base. Once visits rise, the same overhead is spread across more revenue, so margin expands faster than costs. That is why second-year profit can improve sharply, but only if rent and software commitments match realistic capacity. If fixed costs are set for a bigger schedule than the clinic can fill, the owner’s draw stays thin.
Keep Fixed Costs Aligned With Capacity
Track each fixed line monthly and compare it with booked visit capacity, not just actual visits. The key inputs are rent, utilities, insurance, software, cleaning, supplies, and professional fees. If the schedule cannot support those contracts, owner pay gets squeezed even when collections hold up. The fix is simple: keep non-variable commitments tied to the volume the clinic can truly reach.
Before signing, test whether the schedule can absorb the lease and software load. In this model, rent is $12,000 a month, or 59.7% of total fixed overhead ($12,000 / $20,100). That makes lease terms and software seats the biggest control points. If volume is still building, shorter terms and fewer nonessential tools protect cash flow and owner income.
- Watch rent per booked visit.
- Review software seats and contracts.
- Renegotiate before long terms start.
- Cut unused office services fast.
4
Service Mix And Ancillary Revenue
Service Mix Revenue
Service mix matters when each visit is medically necessary, documented, and billable. Preventive visits, chronic care support, nutrition visits, counseling, vaccines, labs, telehealth, and min or in-office procedures can raise revenue per patient without adding many extra rooms, but only if the clinic has the right staffing and billing rules.
In year 3, adding 1 Dietitian and 1 Counselor adds 108 visits/month combined. At assumed prices of $105 and $130, that is roughly $11.3k-$14.0k in monthly charges before payer mix and collections. If coding is weak or the service is not supported by the chart, the cash lift disappears fast.
Track the Mix, Not Just Visits
Measure visits by service line, charge per visit, denials, and collections for GP, Nurse Practitioner, Physician Assistant, Dietitian, and Counselor slots. With 108 ancillary visits/month planned in year 3, every 10% miss is about 11 visits lost, and that cuts owner pay before fixed overhead moves.
- Book preventive and chronic care slots
- Fill labs, vaccines, telehealth
- Document medical necessity every time
- Price by payer and service type
Start new services only when room time, staffing, and billing can support them. The win is higher revenue per patient and better margin, not more risky claims.
5
Revenue Cycle, No-Shows, And Collections
Revenue Cycle Cash
After the visit, cash can still leak. In year one, billing and collections fees run 50% of revenue, or about $31,536, and patient acquisition marketing adds another 30%, or about $18,922. That means a large share of gross revenue is already spoken for before owner pay, so weak collections hit take-home income fast.
Here’s the quick math: if claims, denials, or patient balances slow cash, the clinic still pays rent, staffing, and other fixed costs. No-shows are worse than empty time; they waste provider slots and lower collections without cutting cost. The owner keeps more cash only when visits actually turn into paid claims and collected copays.
Track These
Measure appointment utilization, claim accuracy, denial rate, copay collection, and patient balances every month. Those inputs show if the schedule is turning into cash or just activity. One clean rule: full calendars do not matter if claims bounce or balances age out.
Use this to manage income: fill canceled slots fast, collect copays at check-in, fix coding before submission, and review denials weekly. If utilization rises but collections lag, owner income will not follow. Better cash conversion from the same schedule is the goal.
6
Compare low, base, and high primary care clinic income scenarios
Owner income scenarios
Income swings fast here because capacity, reimbursement, denials, and staffing move together. Base case starts at $630,720 revenue with a first-year operating loss, then turns positive as volume builds.
| Scenario | Low CaseTight cash | Base CaseModeled case | High CaseUpside case |
|---|---|---|---|
| Launch model | This is the slower-growth path with thin collections and owner income pressured by early losses. | This follows the source model: a first-year operating loss, then positive operating profit as volume and staffing scale. | This is the stronger path with better capacity, cleaner collections, and more profit left after overhead. |
| Typical setup | Capacity ramps slower, reimbursement stays lower, denials stay higher, and fixed payroll plus rent keep cash tight. | Year 1 revenue is $630,720 with -$13,895 operating profit before provider compensation, then Year 2 reaches $1,185,615 revenue with $409,073 operating profit before exclusions. | Providers run closer to capacity, denials stay low, marketing stays controlled, and fixed costs are spread across more visits. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Negative to low five figuresSlow start | Loss to $409kCore path | Upper six figuresScale upside |
| Best fit | Use this to test downside cash needs and a weak opening year. | Use this as the core planning case for lender, board, or owner cash planning. | Use this to test what happens if the clinic scales well and cash stays disciplined. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions. Taxes, debt service, reserves, and provider payroll are excluded unless you enter them.
Related Products
- Primary Care Clinic Porter's Five Forces Analysis
- Primary Care Clinic BCG Matrix
- Primary Care Clinic Business Model Canvas
- 7 Critical Financial KPIs for Primary Care Clinic Growth
- Primary Care Clinic Business Plan Template in Pre-Written Word
- 7 Proven Strategies to Boost Primary Care Clinic Profit Margins
- How Much Does It Cost To Run A Primary Care Clinic Monthly?
- Primary Care Clinic Startup Costs: $345K CAPEX And $558K Cash
- Primary Care Clinic Financial Model Template in Excel
- How To Open A Primary Care Clinic In 6–12 Months With Clean Claims
- How to Write a Business Plan for a Primary Care Clinic
- Primary Care Clinic Marketing Mix
- Primary Care Clinic Marketing Plan
- Primary Care Clinic Business Proposal
- Primary Care Clinic PESTEL Analysis
- Primary Care Clinic Pitch Deck Example Editable PPTX
- Primary Care Clinic Business SWOT Analysis
- Primary Care Clinic Value Proposition Canvas
Frequently Asked Questions
In the researched base case, first-year owner distributions are not supported because operating profit is -$13,895 before provider compensation, debt, reserves, and taxes By the second year, operating profit reaches $409,073 before those exclusions on $1,185,615 revenue Actual take-home depends on provider pay, payer mix, debt, and retained cash