 Time to Open12 monthsLaunch runway
Time to Open12 monthsLaunch runwayHow To Open A Radiology Service In 6–12 Months With Payer Readiness

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Time to Open12 monthsLaunch runway  Launch Sequence8 stagesCompliance first
Launch Sequence8 stagesCompliance first Key BottleneckBuildout delayApproval path
Key BottleneckBuildout delayApproval path First Revenue StepBooked scansReferral to bill
First Revenue StepBooked scansReferral to bill


To open a radiology service in the United States, choose the modality mix, confirm state radiation and facility rules, secure a shielded site, install imaging equipment, set up PACS/RIS, hire licensed staff, complete accreditation and payer enrollment, and test scheduling-to-report workflows before the first patient A practical launch window is 6–12 months, but CT, MRI, certificate-of-need review, construction, accreditation, and payer delays can push it longer In the researched Year 1 model, the center starts with 1 radiologist, 1 MRI technologist, 1 CT technologist, 2 X-ray technologists, and 1 sonographer, with modeled monthly revenue near $216,800 at planned capacity The first revenue step is simple: turn referral relationships into scheduled, billable scans with payer-ready claims and fast report turnaround
Time to Open12 monthsLaunch runwayLaunch Sequence8 stagesCompliance firstKey BottleneckBuildout delayApproval pathFirst Revenue StepBooked scansReferral to billRadiology launch timeline
This is a short web summary of the launch plan; the XLSX export contains the detailed Gantt Chart.
Launch scheduleMonth 1Month 2Month 3Month 4Month 5Month 6Month 7Month 8Month 9Month 10Month 11Month 12
Licensing / compliance
- Scope review
- License filing
- Shielding review
- Accreditation file
Site / buildout
- Lease close
- Shielding design
- Renovation work
- Room signoff
Equipment / systems
- Vendor quotes
- Scanner orders
- System buildout
- Acceptance testing
Staffing / training
- Core hires
- Credential checks
- Workflow training
- Drill coverage
Accreditation / payers
- Physicist testing
- Accreditation submission
- Payer enrollment
- Billing setup
Marketing / go-live
- Referral list
- Launch materials
- Outreach campaign
- Go-live review
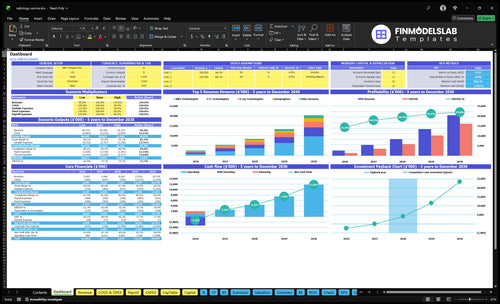
Why test a Radiology Service model before opening?
The Radiology Service Financial Model Template screenshot maps revenue, costs, cash needs, assumptions, and break-even—open it now.
Financial model highlights
- Launch timing and ramp
- Volume, payer, modality mix
- Runway and break-even path
What are the requirements to open a radiology center?
To open a Radiology Service, lock licensing and site feasibility before signing a lease: state radiation control registration, applicable facility licensing, certificate-of-need review in some states, HIPAA, OSHA, and payer enrollment all affect launch timing. For operating focus, tie readiness to What Is The Most Critical Metric For Radiology Service Success?, because a 24-hour report target only works after testing, staffing, and workflow are live.
Required approvals
- Confirm state radiation control registration
- Check facility licensing rules
- Review certificate-of-need where applicable
- Enroll payers before billing
Opening checklist
- Name a radiation safety officer
- Appoint a medical director
- Complete physicist surveys and acceptance testing
- Staff 6 Year 1 clinical roles
How long does it take to open a radiology center?
A Radiology Service usually takes 6–12 months to open, and the timeline is driven by site buildout, shielding design, equipment lead times, physicist testing, accreditation, staffing, and payer credentialing. Here’s the quick math: the room must be ready before equipment can be accepted, and claims may not pay until enrollment is complete. In certificate-of-need states, launch can slip longer, and Year 1 capacity is often only 50%–60% as referrals ramp.
Build first
- Room readiness comes first.
- Shielding design can delay buildout.
- MRI and CT need extra power.
- HVAC and inspections add time.
Launch after setup
- Physicist testing must clear first.
- Accreditation comes before full volume.
- Payer credentialing affects cash flow.
- Referrals take time to ramp.
How do radiology centers get patients before first revenue?
Radiology Service gets patients before first revenue by lining up referral sources first: primary care, orthopedics, urgent care, pain management, employers, attorneys where appropriate, and self-pay, while also planning startup costs like What Is The Estimated Cost To Open And Launch Your Radiology Service Business?. First revenue starts when scans are scheduled and billable, not when marketing begins. Year 1 can be modeled at 100 MRI, 120 CT, 500 X-rays across 2 X-ray technologists, plus 130 ultrasounds and 150 radiologist reads, but trust only sticks if quality and speed hold up.
Build referral flow first
- Target primary care and orthopedics
- Add urgent care and pain management
- Use employer and attorney referrals
- Offer self-pay for direct access
Make orders easy to send
- Support payer access before launch
- Keep scheduling fast and clean
- Help with authorizations upfront
- Turn reports fast, ideally within 24 hours
Confirm whether the imaging center is ready to accept patients
Launch readiness checklist
Use this go-live approval checklist to confirm the radiology service is ready to open before launch.
License and safety
- State radiation registrationCritical
No scan work should start without state radiation approval.
- Facility license confirmedCritical
Confirm any required facility license before opening.
- HIPAA and OSHA controlsCritical
Privacy and workplace safety gaps can stop launch fast.
- RSO namedHigh
A named radiation safety officer owns dose and incident controls.
- Medical director appointedHigh
Clinical oversight needs one accountable physician.
Site and build
- Lease signedCritical
You need the site locked before build-out spend starts.
- ADA access verifiedHigh
Patients must reach the site without access barriers.
- MRI safety zones postedCritical
Controlled MRI zones reduce magnet and screening risk.
- Shielding design approvedCritical
Shielding has to match scan rooms before installation.
- Power and HVAC readyCritical
Scanners and cooling fail fast if power or HVAC is short.
Equipment and systems
- Core scanners deliveredCritical
MRI and CT units need to land before testing starts.
- X-ray and ultrasound installedHigh
All booked modalities must be in place for first patients.
- PACS and RIS liveCritical
Picture archiving and communication system and radiology information system must move images and orders cleanly.
- Billing and clearinghouse readyCritical
Claims must flow before the first payer submission.
- Service contracts signedHigh
Fast repair coverage protects uptime in the first month.
Clinical staffing
- Radiologists scheduledCritical
Report coverage has to match booked scan volume.
- Technologists credentialedCritical
Only licensed staff should run imaging work.
- Front desk staffedHigh
Check-in, phones, and records need an owner on day one.
- Billing partner activeHigh
Revenue cycle management (RCM) partner keeps claims and follow-up moving.
Patient flow
- Referral intake testedHigh
Referrals need a clear path into scheduling and triage.
- Physician outreach launchedHigh
Referring doctors drive first-volume scans.
- Self-pay process readyMedium
Cash-pay patients need a clean quote and pay step.
- Operations playbook signedCritical
The SOP should cover scheduling, auth, consent, contrast, emergencies, and turnaround.
Cash and go-live
- Year 1 volume model checkedCritical
Test the 50%–60% capacity case and ~$216.8k monthly revenue.
- Scan costs at 19%High
Keep scan-linked costs near the modeled 19% level.
- Cash covers Month 5 troughCritical
Minimum cash is -$1.587M in Month 5, so funding must cover it.
- Go-live signoff completeCritical
Do not open if payer, equipment, safety, or reporting steps are still broken.
Want to check the six main radiology launch drivers?
1Regulatory Path
License gateMissing state filing, facility approval, or accreditation can block opening and billing.
2Site Readiness
Shielding readyWrong site or shielding can delay installation and force redesign before opening.
3Equipment Setup
Install timingLate equipment delivery or failed acceptance testing leaves rooms idle at go-live.
4Staff Coverage
6 rolesCoverage gaps slow throughput, hurt report quality, and trigger rescheduled patients.
5Billing Setup
Claims readyUnready payer setup delays first cash, even after scans start.
6Referral Flow
50-60% capWeak referral flow keeps Year 1 at 50% to 60% capacity instead of full rooms.
Regulatory, Licensing, And Accreditation Pathway
Regulatory, Licensing, And Accreditation
For a radiology center, this step is binary: if the state radiation filing, required facility license, certificate-of-need, or payer-recognized credentials are missing, you may not open or bill on day one. That means the room can be built, but the business still cannot serve patients or collect cash.
This path also includes HIPAA and OSHA policies, a named radiation safety officer, a medical director, and a modality accreditation plan. A gap in any of those can slow go-live, delay payer enrollment, or force a last-minute reset after the equipment and staff are already in place.
Lock The Compliance Chain Early
Build a tracker for every license, filing, and payer credential, then tie each item to an owner and due date. Keep the license tracker, payer credential list, safety manual, and quality assurance process in one launch file so nothing gets missed during opening week.
Verify the dependencies before you schedule go-live: equipment specs, physicist reports, and all staffing licenses. If those lag, accreditation and payer setup can stall together, which creates empty scan slots, delayed billing, and avoidable reschedules from day one.
- State filing before patient bookings
- Accreditation before payer claims
- Policies before staff training
- Licenses before final onboarding
1
Site, Construction, And Shielding Readiness
Site, Buildout, and Shielding
This is the first hard gate for opening. A bad site can delay installation, force redesign, or block inspection, so ADA access, patient flow, equipment delivery path, power, and HVAC all need to work before the lease is final. For MRI, CT, and X-ray, room size and shielding are not nice-to-haves; they decide whether the center can open on time.
One missed shield review can turn into a buildout reset. MRI safety zones, CT room planning, X-ray shielding design, and physicist review must line up with landlord approvals and vendor timing. If the signing happens before shielding review, the risk is simple: the room may not pass, equipment acceptance slips, and opening-month surprises hit cash and patient scheduling.
Check the room before you lock the lease
Run a site walk, then sequence the work in the right order: shielding plan, construction schedule, landlord approvals, vendor coordination, and inspection readiness. That keeps the build tied to the actual imaging mix, not guesswork. It also helps avoid late changes that can push equipment delivery and first scans.
- Confirm ADA access first.
- Map equipment delivery paths.
- Review shielding before signing.
- Match HVAC to modality needs.
- Document physicist sign-off.
Build the room for acceptance, not just appearance. If the site is ready, the installation team can move faster, inspectors have fewer issues, and day-one operations are more likely to start cleanly.
2
Imaging Equipment And Vendor Execution
Equipment Delivery and Go-Live Setup
Imaging equipment has to arrive, install, calibrate, and pass acceptance testing before you can scan patients. For a mixed site, the launch depends on the exact modality stack, plus uptime support. If the room is not ready when equipment arrives, the machine can sit idle and opening slips.
The day-one signal is simple: signed equipment quotes, service contracts, a delivery calendar, an installation plan, and PACS/RIS implementation. Year 1 pricing assumptions are MRI at $1,500 per scan, CT at $800, X-ray at $150, ultrasound at $400, and radiologist reads at $200, so lost usable scan capacity hits revenue fast.
Lock the Vendor Sequence Early
Start with the install order, not the purchase order. Verify room readiness, delivery path, power, and the vendor’s acceptance test before you set a go-live date. Then match service coverage to each modality so a missed calibration does not stop first-day scans.
- Confirm delivery and install dates.
- Test PACS/RIS before opening.
- Assign one owner per vendor.
What this hides: a late install can force rescheduling, extra rent burn, and a weak first month because staff are paid before the rooms produce scans.
3
Staffing, Clinical Coverage, And Workflow Readiness
Staffing and Coverage Readiness
Staffing is a day-one gate, not a back-office task. This center needs 1 radiologist, 1 MRI technologist, 1 CT technologist, 2 X-ray technologists, and 1 sonographer in the Year 1 model. If coverage is thin, scan slots go unused, report turnaround slips, and patients get rescheduled before the first week is over.
The key dependency is having licensed staff, signed credential files, and a real coverage schedule before opening. Radiologist coverage also has to line up with medical director oversight and payer enrollment, or the center may be open operationally but not ready to bill or release reports cleanly.
Verify Coverage Before Go-Live
Build the roster, then test the workflow. Before opening, confirm license checks, credential files, front desk training, billing handoff, contrast and emergency protocols, and report turnaround standards. Also confirm PACS/RIS access so images, orders, and reports move without manual workarounds.
Here’s the quick read: one missing technologist or a weak backup plan can slow throughput on every modality. Use a written coverage grid, assign same-day escalation contacts, and test a full patient path from check-in to report release. That’s what cuts first-day delays and keeps reschedules down.
- Confirm license status for every hire.
- Match shifts to modality demand.
- Train front desk on patient flow.
- Test contrast and emergency steps.
- Set report turnaround targets in writing.
4
Payer Enrollment, Billing, And Revenue Cycle Readiness
Billing and payer setup
Open doors do not equal cash in imaging. If Medicare setup, Medicaid where relevant, commercial payer status, and prior authorization rules are not live, scans can happen but claims stall. That pushes first collections out, even when patients are already scheduled. For a radiology site, billing readiness is part of opening on time, not an afterthought.
Year 1 scan-linked costs total 19% before fixed and labor costs. With a $15,000/month lease and $2,500/month utilities, delayed enrollment or weak denial follow-up can strain cash fast. The first revenue only helps if CPT coding, patient estimates, and claim submission work on day one.
Pre-bill before first scan
Build the revenue cycle in this order: payer credentialing, prior authorization rules, CPT code map, patient estimate scripts, clearinghouse testing, then a denial tracker. One clean claim flow beats fast scanning. If the team cannot price, submit, and fix claims quickly, opening dates look good on paper but cash arrives late.
Verify these inputs before launch:
- Medicare enrollment complete
- Medicaid status confirmed where needed
- Commercial payer status tracked
- Prior auth workflow assigned
- CPT coding workflow tested
- Clearinghouse files accepted
- Denial owner named
5
Referral Pipeline And First-Patient Acquisition
Referral Pipeline
For a radiology center, first revenue depends on trusted referral sources, payer access, and scheduling speed. If primary care, orthopedics, urgent care, and pain management offices are not already warmed up, the scanner can open on time and still sit idle in month one.
Plan for 50%–60% ramped capacity in Year 1, not full rooms. That means the launch win is not just opening the doors; it’s having orders, intake, and report flow ready so day one can turn referrals into scans without delay.
Pre-Open Referral Setup
Build the outreach list early and lock the handoff process before opening. Verify referral agreements or commitments, order intake, authorization support, a 24-hour report turnaround promise, and a self-pay pricing path. If any one of those breaks, the patient may get lost between the doctor’s order and the scan slot.
- Confirm target referrers by specialty.
- Test fax, e-order, and call intake.
- Map prior auth responsibilities.
- Set report delivery timing.
- Train staff on self-pay quotes.
What this hides: weak referral conversion can make a fully built site act like it’s half open. One clean one-liner: no referral flow, no first-month revenue.
6
Related Products
- Radiology Service Porter's Five Forces Analysis
- Radiology Service BCG Matrix
- Radiology Service Business Model Canvas
- 7 Core KPIs to Drive Radiology Service Profitability
- Radiology Service Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Radiology Service Profitability
- Analyzing Monthly Running Costs for a Radiology Service
- Radiology Service Startup Costs: $328M CAPEX Opening Plan
- Radiology Financial Model Template in Excel
- How Much Does A Radiology Service Owner Make? $200K Salary Plus Cash Flow
- How to Write a Radiology Service Business Plan: 7 Actionable Steps
- Radiology Service Marketing Mix
- Radiology Service Marketing Plan
- Radiology Service Business Proposal
- Radiology Service PESTEL Analysis
- Radiology Service Pitch Deck Example Editable PPTX
- Radiology Service Business SWOT Analysis
- Radiology Service Value Proposition Canvas
Frequently Asked Questions
Start by choosing the modality mix, then confirm state radiation rules, facility licensing, shielding needs, accreditation, staffing, PACS/RIS, and payer enrollment The researched Year 1 model uses 1 radiologist, 1 MRI technologist, 1 CT technologist, 2 X-ray technologists, and 1 sonographer Use those roles to build your first operating schedule