 Owner income$1.53M-$16.31M
Owner income$1.53M-$16.31MHow Much Does A Radiology Service Owner Make? $200K Salary Plus Cash Flow

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description

Owner income$1.53M-$16.31M  Net margin5.9%-8.0%
Net margin5.9%-8.0% Revenue for target pay$879k
Revenue for target pay$879k Business difficultyHard
Business difficultyHard


Key Takeaways
- Utilization drives owner pay; break-even is about 193 scans.
- MRI pays more, but mix changes total revenue.
- Collected revenue matters more than billed charges.
- Authorization delays and no-shows cut completed services.
Owner income$1.53M-$16.31MNet margin5.9%-8.0%Revenue for target pay$879kBusiness difficultyHardWant to test your owner pay?
Owner income calculator
Estimate owner take-home and target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. It is not guaranteed salary, tax advice, or owner distribution advice.
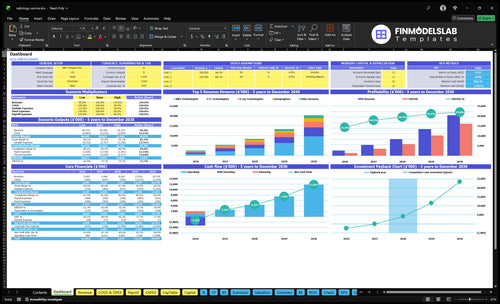
How do you check owner income in the financial model?
The screenshot in the Radiology Service Financial Model Template shows revenue, margin, costs, reserves, and owner take-home assumptions—open the model.
Owner-income model highlights
- Owner take-home output
- Modality revenue and payer mix
- Scenarios and monthly cash flow
- Equipment and staffing costs
How much revenue does a radiology service make?
If you’re asking what a Radiology Service makes, the answer is revenue, not profit: about $26M in year 1, or roughly $2.168M per month, and about $204M in a mature year, or $17M per month. Revenue comes from fee-for-service imaging like MRI at $1,500, CT at $800, X-ray at $150, ultrasound at $400, and reads at $200. Utilization drives realized sales, so volume is the main lever.
Year 1 revenue mix
- $26M first-year revenue
- About $2.168M per month
- MRI prices at $1,500
- CT, X-ray, ultrasound, and reads
Scale case
- $204M mature-year revenue
- About $17M per month
- Utilization drives realized sales
- Revenue rises with more scan volume
What is a radiology service profit margin after operating costs?
Radiology Service can show a 537% first-year modeled margin after operating costs, but that’s only true if utilization holds and the cost stack stays clean. For launch context, see What Is The Estimated Cost To Open And Launch Your Radiology Service Business? The pressure points are real: admin payroll is 19% of revenue, fixed overhead is $255K per month, and financing, service contracts, denials, and radiologist coverage can shrink take-home fast.
Margin drivers
- 537% modeled first-year margin
- 19% admin payroll share
- Margin improves with utilization
- Fee-for-service revenue model
Margin risks
- $255K monthly fixed overhead
- Equipment financing can cut cash
- Service contracts lower take-home
- Denials and coverage gaps hurt
How much can a radiology service owner make?
A Radiology Service owner can model $200K in CEO pay, plus possible distributions if operating cash flow holds; the first-year modeled cash flow is $14M before taxes, debt, reserves, and unlisted equipment or clinical costs. There’s no guaranteed salary, so owner income should be tied to scan volume, payer contracts, modality mix, and What Is The Most Critical Metric For Radiology Service Success?.
Owner Pay
- $200K modeled CEO salary
- Possible cash distributions
- No guaranteed owner salary
- Higher pay needs steady volume
Income Drivers
- $14M modeled first-year cash flow
- Before taxes and debt
- Before reserves and equipment
- Depends on payer and modality mix
Want the six income drivers?
1
750/moScan Volume
At 750 monthly services, more booked scans spread the $25.5K monthly overhead faster and lift EBITDA.
2
10xModality Mix
MRI pays $1,500 versus $150 for X-ray, so mix shifts move revenue faster than raw scan count.
3
4.4MCollections
On a $4.4M first-year revenue base, cleaner billing and collections keep cash from leaking out after the 19% variable cost.
4
6-22 FTELabor Cost
Clinical staffing grows from 6 to 22 FTE, so payroll has to rise slower than revenue or margin gets squeezed.
5
$3.3MEquipment Load
The scanner and buildout stack is about $3.3M, so financing terms and uptime decide how much EBITDA becomes cash.
6
60%-80%Referral Flow
Keeping utilization in the 60%-80% band depends on referrals and authorizations; empty slots don't pay.
Radiology Service Core Six Income Drivers
Scan Volume And Equipment Utilization
Scan Volume And Utilization
With heavy fixed costs, scan volume and equipment utilization are the first owner-income lever. The first-year model shows 571 completed services per month and about $2,168K revenue; break-even with owner pay is about 193 services per month. One empty slot still carries rent, payroll, insurance, and software cost, so idle time hits profit fast.
For MRI, utilization starts at 50% and rises to 80%. The key inputs are completed services, open slots, and fixed monthly costs. Here’s the quick math: stay above 193 services per month and owner pay can be funded; slip below that, and cash flow tightens even if the clinic looks busy.
Fill More Slots
Track completed services per month by modality and compare it to open capacity. Measure MRI fill rate separately, since moving from 50% to 80% is the clearest profit lift. Also watch no-shows, authorization delays, and same-day reschedules, because they decide whether the machine earns or sits idle.
Use a weekly slot report and push fast rebooking. If volume drifts toward 193 services per month, owner draw gets squeezed; if it holds near 571 completed services, fixed costs spread better and take-home income improves. Every unused slot still absorbs lease, payroll, insurance, and software cost.
1
Modality Mix And Reimbursement Weight
Modality Mix And Reimbursement Weight
Revenue per scan changes fast when the mix shifts. In year one, MRI prices at $1,500, CT at $800, ultrasound at $400, and X-ray at $150, so average revenue per completed service is just the weighted mix. The owner’s take-home depends on that mix, not just total scan count.
Higher reimbursement does not always mean higher profit. MRI can bring more dollars per scan, but it also ties up schedule time, equipment, contrast, and staff differently than X-ray or ultrasound, so the best mix is the one with the strongest contribution after direct labor and operating costs.
Track Mix, Not Just Volume
Use this math: (MRI x $1,500 + CT x $800 + ultrasound x $400 + X-ray x $150) / total completed scans. Track completed scans by modality, denial rate, and staff hours by modality so you can see which mix lifts collected revenue and which one only looks good on paper.
- Watch revenue per scheduled slot.
- Compare staff time by modality.
- Flag contrast-heavy cases.
- Test mix against cash flow.
If a higher-MRI month raises revenue but also pushes overtime or slows access, owner draws can fall even with stronger top-line sales.
2
Payer Mix, Collections, And Denials
Collections Over Charges
For a radiology center, income is set by collected revenue, not billed charges. Payer contracts, prior authorization, denials, and days to collect decide how much cash lands in the bank, so the same scan volume can produce very different owner pay. First-year pricing ranges from $150 per X-ray to $1,500 per MRI, but slow payment can still force reserves.
Net collections rate means cash collected divided by what you billed. If denial rate is high or prior auth slows the claim, revenue may look strong on paper while cash stays tight. That matters because fixed costs and payroll keep coming, and the owner’s draw should come from cash, not uncollected claims.
Track Net Cash, Not Gross Billings
Build the model with editable inputs for payer mix, denial rate, and collection speed. Use collected revenue by modality, then test what happens if payers pay slower or reject more claims. That shows whether the business can cover rent, labor, and reserves before the owner takes profit.
- Track denial rate by payer.
- Track days from scan to cash.
- Track prior auth approval rate.
- Track collected revenue by service.
If collections slip, hold more cash. Even with strong scan volume, slower reimbursement can delay distributions and make a profitable month feel short on cash.
3
Radiologist Coverage And Clinical Labor
Clinical Labor Load
Radiologist coverage and clinical labor set the labor floor for the imaging center. The model scales from 1 to 4 radiologists, 1 to 5 MRI technologists, 1 to 4 CT technologists, 2 to 6 X-ray technologists, and 1 to 3 sonographers. When coverage expands faster than completed scans, operating profit drops and owner pay gets squeezed.
Admin payroll starts at $405K, so this is already a heavy fixed-cost layer. Here’s the quick math: more staffed coverage only helps if it raises completed services, cuts wait times, and protects turnaround speed. Owner-operator work should be kept separate from paid labor, or the margin will look better than the cash flow really is.
Track Staffed Hours vs. Completed Scans
Measure labor by staffed shifts, completed scans, and report turnaround. Track radiologist coverage, tech coverage by modality, and admin hours against monthly volume. Use those inputs to test whether the added labor supports more revenue or just adds payroll. If volume does not move, the extra coverage is cost, not capacity.
- Track coverage by modality.
- Separate owner time from payroll.
- Watch admin payroll against volume.
- Test staffing only with demand growth.
What this estimate hides is labor inefficiency from no-shows, slow authorization, and uneven case mix. If MRI or CT demand is thin, a larger coverage team can drag cash flow even with good pricing. The clean test is simple: each added paid role should lift completed services enough to cover its share of fixed labor and keep owner distributions intact.
4
Equipment, Facility, And Maintenance Costs
Facility And Maintenance Burn
For an outpatient imaging site, this driver is the fixed monthly cash load before the owner gets paid. The known spend is about $58.8K/month from $15K lease, $25K utilities, $12K maintenance, $3K insurance, $800 software, $1K compliance, and $2K marketing, before equipment leases, loans, service contracts, shielding, and reserves.
This cost base cuts distributions fast because it is paid whether the center runs at 60% or 90% of capacity. The key input is completed scan volume versus fixed cost per scan. If volume slips, each scan has to carry more overhead, so owner take-home drops even when revenue per scan looks healthy.
Control The Fixed-Cost Load
Track fixed cost per completed scan every month: total facility and maintenance cash cost divided by completed scans. That tells you if the site can still fund profit and owner pay. Keep a separate line for equipment obligations and reserves, because those are cash items, not just accounting expenses.
Cut waste where it matters most: renegotiate the lease, watch utility spikes, use preventive maintenance, and match service contracts to actual equi pment use. If a scanner is down or shielding work is due, a reserve keeps distributions from being forced down at the worst time.
5
Referral Pipeline And Authorization Workflow
Referral Flow And Prior Auth
Completed scans drive income, not raw referrals. If physicians, urgent care, orthopedics, and other outpatient sources send orders but authorization delays or no-shows block the visit, the business loses billable volume and cash flow drops. The first-year plan needs 571 monthly completed services, then scales to 3,174 monthly services, so every lost slot pushes owner pay lower.
Here’s the quick math: revenue only shows up when the scan is done, scheduled fast, and cleared to bill. Slow auth work hurts MRI, CT, X-ray, and ultrasound capacity because open slots expire. That means weaker utilization, more wasted staff time, and less margin to cover fixed overhead before any owner draw.
Track Referrals To Completed Scans
Measure the full funnel: referrals received, orders approved, visits scheduled, scans completed, and no-shows. The key ratio is completed scans per referral source, because a busy feeder channel that stalls in prior auth does not pay the bills. Keep an eye on approval time, schedule fill speed, and same-day reschedules.
Use a simple control sheet by source: physicians, urgent care, orthopedics, and other outpatient providers. The goal is to protect capacity, not just add leads. If scheduling slows, the loss shows up first in idle modality time and then in lower monthly revenue, weaker gross margin, and less cash available for the owner.
- Track auth turnaround time
- Track no-show rate by source
- Track completed scans per referral
- Protect open slots daily
6
Scenario objective for radiology service owner income planning
Owner income scenarios
Owner income rises as imaging volume, staffing, and equipment use move from launch to steady use. This table shows how the model's first-year, base, and mature setups change cash flow.
| Scenario | Low CaseLow case | Base CaseBase case | High CaseHigh case |
|---|---|---|---|
| Launch model | Lower earnings path based on the first operating year. | Modeled earnings path from the third operating year. | Stronger earnings path from the mature year. |
| Typical setup | The model uses 571 monthly services, $26M revenue, a 537% modeled margin, and a $200K CEO salary, with about $14M pre-tax cash flow before debt and reserves. | The model uses 1,529 monthly services, $84M revenue, a 729% margin, and about $62M in pre-tax cash flow before debt and reserves. | The model uses 3,174 monthly services, $204M revenue, an 805% margin, and about $164M in pre-tax cash flow before debt and reserves. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | $14MLow income | $62MBase income | $164MHigh income |
| Best fit | Use this to stress-test the launch year if volume builds slowly or staffing runs light. | Use this as the main planning case if the clinic reaches steady utilization by year 3. | Use this to test upside if volume scales hard and the site runs near full capacity. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Radiology Service Porter's Five Forces Analysis
- Radiology Service BCG Matrix
- Radiology Service Business Model Canvas
- 7 Core KPIs to Drive Radiology Service Profitability
- Radiology Service Business Plan Template in Pre-Written Word
- 7 Strategies to Increase Radiology Service Profitability
- Analyzing Monthly Running Costs for a Radiology Service
- Radiology Service Startup Costs: $328M CAPEX Opening Plan
- Radiology Financial Model Template in Excel
- How To Open A Radiology Service In 6–12 Months With Payer Readiness
- How to Write a Radiology Service Business Plan: 7 Actionable Steps
- Radiology Service Marketing Mix
- Radiology Service Marketing Plan
- Radiology Service Business Proposal
- Radiology Service PESTEL Analysis
- Radiology Service Pitch Deck Example Editable PPTX
- Radiology Service Business SWOT Analysis
- Radiology Service Value Proposition Canvas
Frequently Asked Questions
The model carries $200K in annual CEO pay and about $14M in first-year operating cash flow after listed costs That cash flow is before taxes, debt service, reserves, equipment financing, and any unlisted clinical compensation It is a planning estimate, not guaranteed owner income