How to Open a Nursing Home: 12–24+ Month Launch Plan
Nursing Home Bundle
To open a nursing home in the United States, plan for market validation, entity setup, state licensing, facility inspections, staffing, clinical policies, vendor contracts, payer setup, and compliant resident admissions A practical opening timeline is often 12–24+ months, but state rules, facility condition, certificate-of-need laws, bed count, services, and payer mix can move that timeline In the Year 1 planning case, monthly revenue per resident is about $5,310 before payer delays, based on base residency, assisted living, skilled nursing, and ancillary service assumptions The main bottleneck is survey readiness: the building, staff schedule, records, infection-control plan, and admission process all need to work before first revenue starts
Time to Open12-24 monthsLaunch runwayLaunch Sequence6 stagesCompliance firstKey BottleneckLicense gateState rulesFirst Revenue StepResident admissionBilling live
Launch timeline
This web view shows a short launch summary, and the XLSX export carries the full task-level Gantt chart.
Why test a financial model before opening a Nursing Home?
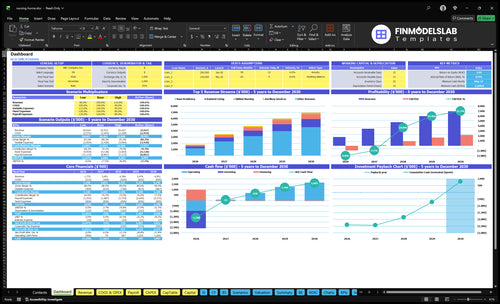
Dashboard tabs map opening month, occupancy ramp, payer mix, staffing, payroll timing, cash runway, and break-even; open the Nursing Home Financial Model Template.
Financial model highlights
Startup costs and timing
Revenue by payer mix
Staffing before full census
What launch mistakes put a nursing home at risk?
If a Nursing Home underbuilds staffing, treats licensing like paperwork, or opens before clinical workflows are ready, it can stall fast. In Year 1, direct care planning starts at 40 hours per resident per month and rises later, so staffing has to follow acuity, not just beds; a basic launch team includes an Executive Director, Director of Nursing, 3 RNs, 8 CNAs, and an Activities Director.
Launch blockers
Failed inspections stop admissions.
Nurse and CNA gaps slow care.
Medication procedures must be complete.
Infection control needs day-one readiness.
Must-have setup
Vendor contracts in place early.
Billing setup ready before move-in.
Resident records complete at launch.
Mock survey before any admissions.
How do you get residents for a nursing home?
Residents usually come from hospital discharge planners, case managers, physicians, elder-law attorneys, Medicaid offices, senior placement agencies, and local family outreach, but a Nursing Home should only admit after licensing, survey readiness, payer setup, and the admission workflow are cleared. With a $250,000 year-one marketing budget and a $4,500 CAC (customer acquisition cost), the model points to about 55 resident acquisitions if the channel mix performs as planned. First revenue still depends on qualified residents, signed admission documents, payer eligibility, care-plan documentation, and billing setup; for cost context, see How Much Does It Cost To Open A Nursing Home Business?
Top referral sources
Hospital discharge planners drive early referrals.
Case managers steer care placement.
Physicians add trusted referrals.
Elder-law attorneys and families help fill beds.
Admit only when ready
Clear licensing before admitting anyone.
Finish survey readiness first.
Set payer billing and eligibility rules.
Match occupancy ramp to staffing and acuity.
How long does it take to open a nursing home?
Open a nursing home in 12–24+ months in most cases, and longer if you need new construction, major renovation, or state review. The fastest path is an already compliant facility with experienced operators; the slowest path is a new build or any market with certificate-of-need review. Life-safety inspections, staffing, policy docs, payer enrollment, and survey timing all sit on the critical path, so plan cash for pre-opening payroll and fixed costs like rent, insurance, software, legal, and maintenance.
Timing drivers
12–24+ months is the usual range
New construction takes the longest
Renovation adds review and inspection time
State survey timing can delay opening
Early cost setup
Carry pre-opening payroll in Year 1
Fund rent, insurance, and software early
Include legal and maintenance before residents arrive
Stage readiness by opening month and ramp-up
Nursing Home Financial Model
5-Year Financial Projections
100% Editable
Investor-Approved Valuation Models
MAC/PC Compatible, Fully Unlocked
No Accounting Or Financial Knowledge
Confirm the nursing home is legally and operationally ready to accept residents
Launch readiness checklist
Use this go-live approval checklist to confirm the nursing home is ready before opening.
1Licensing
State license filedCritical
No resident intake should start until the state license path is clear.
Certificate of need reviewedCritical
Some states require this before opening, so it can block launch.
Inspection pass receivedCritical
Passing the pre-opening inspection is the last gate before opening.
2Policies
Resident rights postedHigh
Resident rights must be visible before the first move-in.
Infection control plan approvedCritical
This lowers outbreak risk and supports survey readiness.
Medication policy setCritical
Safe medication handling is a core launch control point.
3Facility
Rooms furnished and safeHigh
Resident rooms need safe furniture, storage, and clear access.
Kitchen laundry fully readyHigh
Food and laundry gaps can stop service on day one.
Security monitoring activeHigh
Active monitoring protects residents, staff, and property.
4Staffing
Executive Director onboardedCritical
This role owns launch decisions and daily accountability.
Nursing coverage roster builtCritical
Coverage must match resident care hours before opening.
Training and orientation completeHigh
Staff need policy and care training before resident intake.
5Vendors
Pharmacy and supplies contractedCritical
Medication and supply gaps can halt care quickly.
EHR and billing liveCritical
The electronic health record and billing system must work on day one.
Waste maintenance insurance activeHigh
Core service vendors and insurance reduce launch disruption risk.
6Admissions
Intake workflow testedCritical
If intake fails, the facility is open but cannot earn revenue.
Referral channels activeHigh
Hospital and advisor referrals drive the first resident pipeline.
Cash runway verifiedCritical
The model shows early cash strain, so runway must be checked before opening.
Which launch drivers decide whether the nursing home can open?
1Licensing
12-24+ mo
No approval means no admissions, so state review timing sets the launch date.
2Facility Ready
Day-1 pass
Rooms, fire systems, and records must pass inspection before safe day-one care.
3Admin Staffing
40 hrs/res
Hire and train the director, RNs, and CNAs early so coverage matches Year 1 needs.
4Survey Prep
Mock ready
Written protocols and staff drills cut opening deficiencies and speed resident intake.
5Payer Setup
$5.31K/mo
Billing, contracts, and claims files must be live, or occupied beds still delay cash.
6Referral Pipeline
55 admits
A live referral tracker fills beds faster and keeps admissions from stalling after approval.
Licensing and Regulatory Approval
Licensing Gate
For a nursing home, licensing is the gate, not a formality. Without a compliant state approval, you have 0 resident admissions, so the opening date slips and first revenue starts late. This is a hard stop, not a paperwork detail.
The approval file usually includes the state license application, certificate-of-need review where required, administrator credentials, ownership disclosures, facility documents, inspections, and Medicare or Medicaid certification if those payers are part of the plan.
Build the Approval File First
Assign one owner and track every filing, survey, and follow-up date. The main bottleneck is state review timing or a failed survey, so sequence the work around the approval path, not the buildout wish list.
Complete the application before final vendor payments.
Keep ownership and credential files current.
Store inspection evidence in one survey-ready file.
Confirm payer certification before opening.
The readiness signal is a clear approval path, a complete application, a survey-ready file, and one internal owner who can answer questions fast. If any of that is missing, the launch date is too early.
1
Facility and Life-Safety Readiness
Facility Readiness
For a nursing home, the building is part of the care model. Resident rooms, nurse stations, dining, therapy, kitchen, laundry, HVAC, elevators, fire systems, accessibility, security, and infection-control layout all have to work before the first move-in.
The launch gate is simple: the site must be able to pass inspection and support care on day one. A failed fire inspection, missing maintenance records, or a kitchen that is not ready can block admissions even when staffing and payer work are done.
Day-One Check
Finish the physical plant punch list first, then do the life-safety review, lock in maintenance contracts, and document emergency procedures. Test resident flow from entry to dining, therapy, and care areas so staff can catch bottlenecks before opening. No compliant building, no admissions.
Keep inspection records, service logs, and vendor contacts in one file. Verify the kitchen, laundry, HVAC, elevators, and infection-control layout before the opening date, because weak setup here turns into delayed revenue, last-minute fixes, and unsafe first-week operations.
Close punch list before final walk-through.
Test fire and evacuation paths.
Verify kitchen and laundry readiness.
File maintenance and inspection records.
2
Administrator and Clinical Staffing
Clinical Staffing Readiness
When a nursing home opens, staffing is not just an HR task. It is the difference between safe admissions and a launch that falls apart on day one. The visible Year 1 model includes 1 Executive Director at $150,000, 1 Director of Nursing at $120,000, 3 RNs at $85,000 each, 8 CNAs at $40,000 each, and 1 Activities Director at $60,000, or $905,000 before dietary, housekeeping, maintenance, therapy coordination, admissions, and compliance support.
Here’s the quick math: direct care planning is 40 hours per resident per month, which is about 1.33 hours per resident per day. If the licensed leader and nursing team are not hired, trained, and scheduled before move-in, you risk weak coverage, slower response times, and survey problems. Hire too early and cash burns; hire too late and you open with gaps.
Sequence Hires Before Census
Build the roster around the care load, then test the schedule before the first resident arrives. The key is to prove that the administrator or Executive Director, Director of Nursing, RNs, and CNAs can cover shifts, document care, and escalate issues without delay. If training starts after opening, staff will learn on live residents, and that is where avoidable errors show up.
Lock the leader and nursing roles first
Map coverage to resident acuity
Train before first admissions
Document backup coverage by shift
Assign compliance and admissions support
What this setup hides: the extra non-clinical roles still need to be in place to keep meals, cleaning, repairs, therapy coordination, and intake moving. If those support lines are thin, clinical staff spend time fixing process gaps instead of caring for residents.
3
Policies, Procedures, and Survey Readiness
Survey Readiness
Survey readiness is what lets the nursing home open on time because it proves care can run the same way every day, not just look good in a file. The facility needs working clinical protocols, resident rights, admissions procedures, medication management, infection control, staff training, emergency preparedness, quality assurance, incident reporting, and records management before day one.
The real risk is simple: if documentation is thin or staff cannot explain the process, surveyors see gaps fast, and opening deficiencies stack up. That can slow first-resident admissions, make payer enrollment harder, and create avoidable cash burn while the building sits ready but not truly launch-ready.
What to Test Before Opening
Build the policy set in the order staff will use it. Then run mock survey testing and resident intake drills until the team gives the same answers and follows the same steps every time. One clean standard is better than ten binders nobody uses.
Verify admissions and resident rights
Test medication and infection control
Train on emergency response steps
Check incident reporting and records
Walk through quality assurance reviews
Assign one owner to keep every version current. If walk-throughs expose weak spots, fix them before opening, because survey gaps usually come from missing forms, inconsistent handoffs, or staff who know the task but cannot explain it clearly.
4
Payer Setup and Revenue-Cycle Readiness
Payer Setup and Billing Readiness
First revenue depends on clean payer setup. In a nursing home, you can open beds and still not collect if private-pay contracts, Medicaid enrollment, Medicare certification where applicable, and managed-care contracts are not in place. Billing workflow also has to be live on day one, or occupancy turns into unpaid AR.
Here’s the quick math: $3,500 base residency, $2,500 assisted living add-on at 40%, $6,000 skilled nursing at 10%, and $300 ancillary charges at 70% gives about $5,310 per resident per month before collection timing. If you admit before documentation and payer files are ready, cash flow lags even when beds are full.
Set Up Cash Collection Before Move-In
Build the billing path before the first resident arrives. Verify payer packets, eligibility checks, care-plan documentation, claims workflow, denial tracking, and cash collection procedures. Assign one owner for each step so admissions, nursing, and billing do not stall each other during the first month.
Lock private-pay contracts first.
Confirm Medicaid and Medicare files.
Test billing software and eligibility checks.
Standardize care-plan documentation.
Track denials from day one.
What this setup hides is timing risk: a bed can be occupied, but revenue still waits on clean claims and approved payer files. If that workflow is not tested before opening, the business may need extra working capital just to bridge the delay.
5
Referral Network and Resident Admission Pipeline
Referral Pipeline
If the rooms are ready but referrals are not, opening still drifts and beds sit empty. This driver is compliant census-building: hospital discharge relationships, case manager outreach, physician and elder-law attorney ties, senior placement agency setup, family inquiry handling, tours, admissions criteria, payer screening, and intake workflow. A live referral tracker and admission decision process should be live before opening.
The math is simple: $250,000 in Year 1 marketing at $4,500 CAC implies about 55 resident acquisitions if channels convert. If approvals land before demand, you carry staff and fixed costs with empty beds, and that slows cash recovery. If demand arrives without screening, you risk poor-fit admissions and heavier care friction on day one.
Build the referral engine first
Set the intake path before the first tour. The founder should verify who answers inquiries, who screens payer fit, who approves admissions, and how fast each referral source gets a response. One clean rule helps: if the lead is qualified, the next step must be scheduled the same day.
Track source, status, and next action.
Script family calls and tour follow-up.
Pre-approve admissions criteria and payer checks.
Assign hospital and physician outreach owners.
Test intake before opening day.
What this setup hides is timing risk. If the tracker is manual, or if a case manager waits two days for a callback, occupancy ramps slower and staff scheduling gets messy. A tight referral process lets census grow faster without stuffing the building with the wrong mix of residents.
Start with state licensing, facility feasibility, and operator readiness The opening path usually runs 12–24+ months and includes inspections, policies, staffing, payer setup, and referral development Use the Year 1 model to test $5,310 estimated monthly revenue per resident, 40 direct care hours per resident per month, and pre-opening fixed costs
Revenue starts only after approvals, survey readiness, payer setup, and compliant admissions Even then, collection timing depends on private pay, Medicare, Medicaid, or managed-care processes In the planning case, Year 1 revenue per resident is about $5,310 per month before payer timing, while marketing assumes $250,000 and $4,500 CAC
You don’t personally need to be a clinician in every state, but the facility needs qualified leadership and licensed clinical coverage The Year 1 staffing plan includes an Executive Director, Director of Nursing, 3 RNs, 8 CNAs, and an Activities Director State administrator requirements, nurse coverage rules, and resident acuity drive the final staffing plan
Licensing, facility inspections, staffing, and payer enrollment cause the biggest delays Construction or renovation can also push the schedule past the 12–24+ month planning range If the building is not life-safety ready, policies are incomplete, or nurses and CNAs are not trained, admissions should wait even if marketing demand exists
Check licensing feasibility before committing to rent The model carries $45,000 monthly facility lease or rent, plus property taxes and insurance at $12,000 per month, so a bad site decision burns cash fast Confirm zoning, certificate-of-need rules where applicable, inspection needs, staffing access, payer strategy, and referral demand first
About the author
Martin Fletcher
Founder Support Writer
Martin Fletcher is a founder support writer at Financial Models Lab, focused on practical profit planning for founders writing a business plan. He helps small business owners understand how profit works, with clear guidance on startup cost estimates and the numbers to check before money is invested. His writing keeps the focus on useful figures and realistic expectations.
Choosing a selection results in a full page refresh.