 Owner income$356k
Owner income$356kHow Much Do Nursing Home Owners Make? 43-Resident Breakeven

Fully Editable
Instant Download
Professional Design
Pre-Built
No Expertise Is Needed
Description
Owner income$356k  Net margin11.2%
Net margin11.2% Revenue for target pay$3.19M
Revenue for target pay$3.19M Business difficultyHard
Business difficultyHard


A nursing home owner can make meaningful income, but only after census covers a heavy fixed-cost base In the first year assumptions, revenue is about $63,720 per resident per year, variable costs are 21%, and fixed payroll, rent, overhead, and marketing total about $216 million That puts breakeven near 43 average residents before debt service, reserves, taxes, and owner distributions At 50 average residents, operating cash before those items is about $356,000, but that is not guaranteed owner take-home
Owner income$356kNet margin11.2%Revenue for target pay$3.19MBusiness difficultyHardWant to test your nursing home owner pay?
Owner income calculator
Estimate owner take-home and the target-pay gap from revenue, margin, costs, reserves, and target pay.
Planning note: Research-based planning estimate only. Actual owner income depends on census, payer mix, staffing, debt, taxes, and reserve needs. Not guaranteed salary, tax advice, or owner distribution advice.
Want to see the Nursing Home financial model?
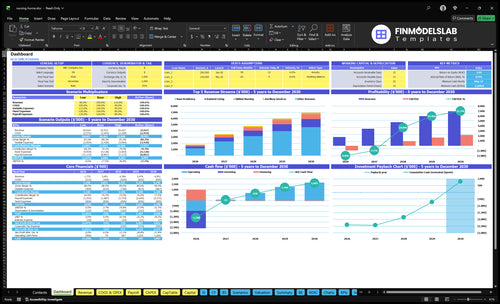
This dashboard ties census, payer mix, staffing, direct care hours, costs, capex, and owner pay capacity in the Nursing Home Financial Model Template, with $4,500 Year 1 CAC built in. Open it to check revenue per resident, breakeven residents, and cash before debt.
Core inputs and outputs
- Scenario income outputs
- Initial capex: $1375 million
- $45k monthly rent
- $12k taxes and insurance
- 40 care hours monthly
How much does a nursing home owner make per year?
A Nursing Home owner does not have a fixed annual take-home; at 50 average residents, the model shows about $356,000 of operating cash before debt, reserves, taxes, and owner distributions. If the owner also serves as Executive Director, keep that $150,000 salary separate from profit distributions, and track census movement with What Is The Current Growth Rate Of Your Nursing Home Business?.
Quick math
- $63,720 annual revenue per resident
- 21% variable costs
- $50,338.80 contribution per resident
- 43 residents to break even before debt
Owner pay drivers
- Census controls cash flow
- Rates set revenue per bed
- Staffing drives fixed payroll
- Debt and reserves reduce distributions
How many beds does a nursing home need to be profitable?
A Nursing Home does not need a fixed bed count to be profitable; it needs enough occupied beds to hit breakeven census. Using $5,310 monthly revenue per resident and a 79% contribution margin, the breakeven point is about 43 average residents, and it rises to about 46 if the owner wants $150,000 before tax. Beds should exceed that number so you can absorb move-outs, payer delays, and staffing gaps.
Breakeven census
- 43 average residents covers breakeven
- $5,310 monthly revenue per resident
- 79% contribution margin drives cash
- Occupied beds matter more than license count
Profit buffer
- 46 residents targets $150,000 before tax
- Keep extra beds for move-outs
- Reserve room for payer delays
- Staffing coverage needs spare capacity
What nursing home expenses reduce owner take-home most?
The biggest owner take-home drains in a Nursing Home are payroll, rent, property taxes and insurance, marketing, and the 21% variable-cost stack from food, supplies, laundry, activities, and utilities. If you’re pricing the model, see How Much Does It Cost To Open A Nursing Home Business? because Year 1 payroll is listed at $1085 million, rent is $45,000 per month, and property taxes plus insurance run $12,000 per month. One clean truth: if agency labor and overtime rise, margin falls fast.
Big fixed costs
- Payroll is the top drain
- Rent is $45,000 monthly
- Insurance and taxes are $12,000 monthly
- Marketing adds $250,000 in cost
Margin leaks
- Variable costs equal 21% of revenue
- Food and supplies hit cash every month
- RN FTE rises from 3 to 7
- CNA FTE rises from 8 to 18
Want to see what moves nursing home owner income?
1
43 resOccupancy
Below 43 residents in Year 1, fixed rent and payroll outrun cash; above it, every filled bed adds margin.
2
$175-$271Payer Mix
Higher-acuity and better-paid residents push revenue per occupied bed day up and lift take-home fast.
3
$1.09M-$1.83MStaffing Cost
Payroll climbs from about $1.09M to $1.83M, so labor control is the biggest guardrail on margin.
4
21%-16%Acuity Mix
As variable costs fall from 21% to 16% of revenue, more of each new resident dollar reaches EBITDA.
5
$45K/moLease Burden
The $45,000 monthly lease is a fixed cash drain, so low census hurts income long before the beds fill.
6
$1.7MCash Buffer
A $1.7M cash trough by Month 17 means slow admissions or compliance problems can force outside funding before payback.
Nursing Home Core Six Income Drivers
Occupancy And Census
Occupancy And Census
Occupancy and census are the same cash driver: how many beds are filled on average. Empty beds still carry rent, leadership, licenses, and core staff, so revenue drops faster than cost does. At $5,310 monthly revenue per resident, or about $63,720 a year, the model shows about 21% variable costs and roughly $50,339 annual contribution per occupied resident.
Here’s the quick math: break-even is about 43 average residents before debt, reserves, taxes, and owner pay. Moving from 43 to 50 residents adds about $352,000 of annual contribution. That is why owner pay rises fastest when census grows and staffing can still protect care quality.
Track Census, Not Just Beds
Track average daily census, move-ins, move-outs, and staffed-bed capacity each month. Use the number of occupied residents, not licensed beds, to forecast cash. If census runs below 43, owner draw should wait because the gap is covering fixed cost, not creating profit.
Manage the driver by matching admissions to labor. More residents help only when RN and CNA coverage can handle care without overtime or quality slips. If staffing lags, the extra census can turn into turnover, agency use, and weaker take-home pay instead of a clean contribution gain.
1
Payer Mix And Rates
Payer Mix And Rates
Revenue here depends on what care each resident buys and what the payer will cover. In the model, base residency is 100%, assisted living is 40% to 60%, skilled nursing is 10% to 30%, and ancillary services are 70% to 90%. That mix lifts blended monthly revenue from $5,310 in Year 1 to $8,246 in Year 5.
Here’s the quick math: higher acuity and more add-on services can raise gross revenue, but only if reimbursement holds. Skilled nursing is priced at $6,000 to $7,000 monthly in the assumptions, yet Medicaid, Medicare skilled stays, managed care, and private pay all vary by state and contract. So this driver changes owner pay by changing revenue per bed, collection timing, and margin.
Track Payer Mix By Bed
Measure monthly census by payer type, service tier, and ancillary attach rate. You need resident count, monthly fees, reimbursement class, and collection lag to forecast cash. If a higher-paying mix needs more staffing or longer authorization cycles, the extra revenue can shrink fast. What matters is net revenue per occupied bed, not just posted rates.
Test rate changes against cash flow, not wishful pricing. Track the share of private pay, Medicaid, and skilled stays, then compare billed revenue to collected revenue each month. If a contract cuts rates or delays payment, owner draw can fall even when census stays flat. The clean target is higher blended revenue without a jump in denials, write-offs, or unpaid days.
2
Staffing Costs
Staffing Costs
Staffing costs are the labor bill for RN and CNA care, plus overtime, benefits, turnover, and agency nurses. In this model, payroll rises from $1.085 million in Year 1 to $1.825 million at maturity, while RN staffing grows from 3 to 7 FTE and CNA staffing from 8 to 18 FTE. That extra $740,000 a year can make even a full building feel cash-poor if census or rates do not keep up.
Direct care hours rise from 40 to 60 per resident per month, so margin depends on staffing to need, not just filling beds. If labor runs hot, owner pay gets squeezed because care and compliance come first, then profit. One clean rule: if payroll rises faster than resident revenue, take-home income falls.
Hold labor to resident load
Measure labor by payroll per resident per month, overtime hours, agency share, and turnover. Those inputs show whether staffing is scaling cleanly or leaking cash. If direct care hours must rise from 40 to 60, forecast the added payroll before you hire, not after the week ends.
Protect margin by matching schedules to census and acuity mix, then watching overtime before it becomes permanent. If agency nurses or turnover push pay above the base model, operating margin drops fast and owner draws wait. Track the staffing plan weekly; don’t let a full building hide a weak labor model.
3
Facility Scale And Acuity Mix
Facility Scale and Acuity Mix
More beds only help when the building fills with the right care mix. A larger facility can spread fixed costs like $45,000 monthly rent and $12,000 monthly property taxes and insurance, plus software, maintenance, and leadership payroll. But a shift in acuity is not free: skilled nursing share rising from 10% to 30% means more staffing, equipment, oversight, and compliance work.
Owner income improves when revenue per occupied bed rises faster than labor and compliance cost. Direct care hours moving from 40 to 60 per resident per month can support higher-acuity revenue, but quality slips hit margin fast through turnover, rework, and survey risk. Bigger is not better if quality drops.
Track Bed Use by Care Level
Measure the mix, not just the headcount. Track occupancy by care level, skilled nursing share, direct care hours per resident, overtime, and agency use. Here’s the quick math: if fixed facility costs already include $57,000 a month in rent, taxes, and insurance before software, maintenance, and leadership payroll, empty beds and weak acuity mix can drain owner pay fast.
- Price higher acuity by cost.
- Track hours per resident monthly.
- Hold quality before adding beds.
Test each census increase against staffing and compliance. If the move from 10% to 30% skilled nursing share does not cover the extra labor and oversight, the extra beds only create busy work, not profit.
4
Real Estate, Debt, And Capital Spending
Real Estate Cash Drag
Operating profit is not the same as cash you can pull out. This model carries $45,000 monthly rent and $68,800 in fixed overhead before payroll and marketing, so EBITDA—earnings before interest, taxes, depreciation, and amortization—can look positive while distributable cash stays tight.
Starting capex totals 1,375 million across medical equipment, kitchen equipment, room furnishings, community furnishings, IT, and security systems. If you add a mortgage or loan, that debt service sits below operating profit and cuts owner pay dollar for dollar. High rent, renovations, and deferred maintenance can still burn cash even with good census.
Track Cash, Not Just Profit
Track cash after rent, overhead, and debt service, not just EBITDA. Here’s the quick check: operating profit minus rent, fixed overhead, and any loan payment is what can fund reserves and owner draw. If that math is thin, the building is cash-poor even when profit looks fine.
Set a capex reserve for replacements and code items, and tie it to asse t age. One clean rule: if the roof, rooms, or systems need work, book the cash need now or it shows up later as a surprise hit to distributions.
5
Compliance, Insurance, And Reserves
Compliance, Insurance, and Cash Reserves
Reserves are not leftover profit. In a nursing home, they cover surveys, fines, legal costs, claims, repairs, and payer delays. The fixed compliance load already includes $12,000 a month for property taxes and insurance plus $3,000 for legal and accounting, so the model starts with $15,000 in monthly overhead before owner pay.
Weak quality control can lift labor costs, create marketing friction, raise liability exposure, and increase turnover. That hits cash twice: more spend now and slower collections later. So even if operating profit looks fine, the owner should not take distributions until reserve needs are funded first.
Fund the reserve before you pay yourself
Track cash, not just profit. Build the reserve off monthly fixed compliance costs, payer delay days, claim exposure, and repair risk. At a minimum, protect the disclosed $15,000 monthly legal, accounting, tax, and insurance burden before owner draws, then add room for surveys, fines, and unexpected fixes.
Use a simple rule in the forecast: reserve funding first, distributions last. If quality slips, assume higher labor, turnover, and legal spend and cut owner take-home fast. That keeps the business liquid and lowers the chance of a cash crisis when reimbursement slows or a repair hits.
6
Scenario objective for low, base, and high nursing home owner-income planning
Owner income scenarios
Resident count, service mix, and staffing drive owner income here. Licensed beds and occupancy were not provided, so the cases use 43, 50, and 60 resident planning points.
| Scenario | Low CaseBreakeven risk | Base CaseCore plan | High CaseUpside |
|---|---|---|---|
| Launch model | This is the lower earnings path with a tight resident count and little room after fixed costs. | This is the modeled middle path with steadier resident volume and owner cash coming through. | This is the stronger earnings path with fuller rooms and more cash after fixed costs. |
| Typical setup | About 43 residents at $5,310 monthly revenue per resident, 21% variable costs, and heavy fixed payroll and overhead leave the model around breakeven before debt, reserves, taxes, and owner pay. | At 50 residents, Year 1 revenue is about $3.186 million and operating cash is about $356,000 before debt, reserves, and taxes. | At 60 residents, Year 1 revenue is about $3.823 million and operating cash is about $860,000 before debt, reserves, and taxes. |
| Cost drivers |
|
|
|
| Owner income rangeBefore owner reserves | Near breakevenNear breakeven | $356,000Cash positive | $860,000Strong cushion |
| Best fit | Use this to test downside cash coverage when census stays soft and owner pay has to wait. | Use this as the working plan if you expect steady admissions and can hold staffing in line. | Use this to test upside when admissions stay strong and staffing stays controlled. |
Planning note: These scenario ranges are researched planning assumptions, not guaranteed earnings, salary promises, tax advice, or distributions.
Related Products
- Nursing Home Porter's Five Forces Analysis
- Nursing Home BCG Matrix
- Nursing Home Business Model Canvas
- 7 Essential Financial KPIs for Nursing Home Operations
- Nursing Home Business Plan Template in Pre-Written Word
- 7 Strategies to Boost Nursing Home Profitability and Margin
- Nursing Home Running Costs: How Much Does It Cost To Operate Monthly?
- Nursing Home Startup Costs: $16M CAPEX And Cash Runway Plan
- Nursing Home Financial Model Template in Excel
- How to Open a Nursing Home: 12–24+ Month Launch Plan
- How to Write a Nursing Home Business Plan in 7 Actionable Steps
- Nursing Home Marketing Mix
- Nursing Home Marketing Plan
- Nursing Home Business Proposal
- Nursing Home PESTEL Analysis
- Nursing Home Pitch Deck Example Editable PPTX
- Nursing Home Business SWOT Analysis
- Nursing Home Value Proposition Canvas
Frequently Asked Questions
Owner salary is not the same as owner profit The assumptions include a $150,000 Executive Director salary, but that may be paid to the owner only if they fill that operating role Distributions come after revenue covers payroll, $45,000 monthly rent, marketing, reserves, debt service if any, and taxes